Download
1 / 23
230 likes | 428 Views
AIOM post ASCO review: updates and news from the Annual Meeting in Chicago Bologna, 19 - 20 giugno 2010. MELANOMA. Ruggero Ridolfi IRST Meldola , Forlì. AIOM post ASCO review: updates and news from the Annual Meeting in Chicago. HIGH LIGHTS: Improved Survival with Ipilimumab

E N D
AIOM post ASCO review: updates and news from the Annual Meeting in Chicago Bologna, 19 - 20 giugno 2010 MELANOMA Ruggero Ridolfi IRST Meldola, Forlì
AIOM post ASCO review: updates and news from the Annual Meeting in Chicago HIGH LIGHTS: Improved Survival with Ipilimumab in Patients with Metastatic Melanoma F. S. Hodi et Al.
AIOM post ASCO review: updates and news from the Annual Meeting in Chicago • Chemotherapy • Carbo+Tax + Sorafenib vs Carbo+Tax + Placebo • 820 Ptz 18% vs 16 % OR NEGATIVO (K. Flaherty) • Local-regional treatment for melanoma hepatic metastases • Melphalan in meta epatiche da melanoma oculare • 29 Ptz ; 62% OR; No >OS (JF. Pingpank) • Immune-Therapy • adjuvant treatment • treatment for stage IV • Targeted Therapies • genomic predictive biomarkers • combinations
Adjuvant treatments • Interferon alpha 2b: PEG-IFN-2b 36months • vs IFNalpha2b 18months. “low dose” PEG-IFN did not show superiority over “low” dose IFNalpha in a population of stage I to IIIb melanoma. Grade 3-4 SAE more frequent in PEG-IFN arm. Treatment in the PEG-IFN arm was not of prolonged duration due to high discontinuation rate. (Grobb JJ et. Al. EADO trial) • GM-CSF +/- peptide vaccination in HLA-A2+ patients or GM-CSF vs placebo in HLA-A2- patients: neither GM-CSF or peptide vaccination achieved significant improvement in OS and DFS. Suggestion of favorable effect of GM-CSF on DFS (0.04), largest in stage IV subjects (subsets analysis). 815 Ptz (Lawson DH.)
Immune-Therapy • TIL + Hd IL-2 • Good Results (MD Anderson –Texas ) • Cytokines • IND 189 study (IL-21): RR 22%, PFS 4.3 months. Inhibits CD8 effector differentiation , • increased secondary expansion (T. Petrella) • Checkpoint blokade • Re-induction with ipilimumab, gp100 peptide vaccine after or a combination of both froma a phase III randomized trial: 40 Ptz (10%) who recieved reinduction: (7/40) durable objective response/ (15/40) stable disease are achieved in subjects who recieved re-induction upon PD. (Hodi)
Targeted Therapies Melanoma Genomics 45% BRAF mutations 25% NRAS mutations 15% PTEN loss • Clinical responses to AZD6244 based combination therapy stratified by gene mutations (Phase I, 25 melanoma pts):AZD6244+DTIC or Docetaxel or Erlotinib or temsirolimus. RR plus chemotherapy 28%. • BRAF mutation: 56% RR (predict clinical benefit?) • NRAS mutation: 0% RR • Wild-type: 0% RR (Patel Sp. Et al.) • Randomized Phase II trial of sorafenib with temsirolimus or Tipifarnib (NRAS farnesyltransferase): only arm A with temsirolimus met the criteria to open second stage accrual with 2 PR and 11 PFS among first 30 accrued. • (Margolin K. Et al) • Phase I/II study of GSK2118436, a selective inhibitor of oncogenic mutant of BRAF Kinase in patients with metastatic melanoma and other solid tumors:AEs most common pyrexia, SAE most common pyrexia and skin squamous cell carcinoma. Confirms target in selective BRAF inhibitors, efficacy in CNS metastases, durability, effecto on survival (?). • (Kefford r. et al)
AIOM post ASCO review: updates and news from the Annual Meeting in Chicago • HIGH LIGHTS CONCLUSIONS….. • Molecular Profiling for ptz selection • BRAF- inhibitors selectivity • Understand Mechanisms of resistance • Combination therapy: • MAPK pathway: BRAF+MEK inhibitors • MAPK pathway+P13K/AKT pathway inhibitors • Selectivity and potency of agents • ……..BUT………
ASCO HIGH LIGHTS STAR Improved Survival with Ipilimumab in Patients with Metastatic Melanoma
MECCANISMI DI IMMUNOSOPPRESSIONE TUMORALE FAS Linfocita T ? FAS - L APOPTOSI p56lck X X TGF- cat X cat CTLA-4 IL-6 X X X CD28 ANERGIA IL-10 ? TCR X VEGF B7 HLA Cellula tumorale Antigene Cellula dendritica Linfocita T CD4+/25+ FoxP3+ immunoregolatore/immunosoppressivo
IL-2 CTLA-4 B7 IL-2 (Activation) CD28 (Blocking) ANERGIA APC T-cell CTLA-4 T-reg
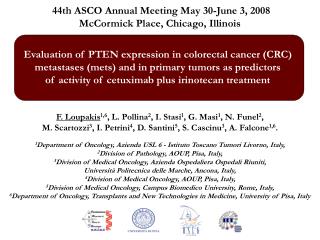
Improved Survival with Ipilimumab in Patients with Metastatic Melanoma F. Stephen Hodi, M.D., Steven J. O'Day, M.D., David F. McDermott, M.D., Robert W. Weber, M.D., Jeffrey A. Sosman, M.D., John B. Haanen, M.D., Rene Gonzalez, M.D., Caroline Robert, M.D., Ph.D., Dirk Schadendorf, M.D., Jessica C. Hassel, M.D., Wallace Akerley, M.D., Alfons J.M. van den Eertwegh, M.D., Ph.D., Jose Lutzky, M.D., Paul Lorigan, M.D., Julia M. Vaubel, M.D., Gerald P. Linette, M.D., Ph.D., David Hogg, M.D., Christian H. Ottensmeier, M.D., Ph.D., Celeste Lebbé, M.D., Christian Peschel, M.D., Ian Quirt, M.D., Joseph I. Clark, M.D., Jedd D. Wolchok, M.D., Ph.D.,Jeffrey S. Weber, M.D., Ph.D., Jason Tian, Ph.D.,Michael J. Yellin, M.D., Geoffrey M. Nichol, M.B., Ch.B., Axel Hoos, M.D., Ph.D., and Walter J. Urba, M.D., Ph.D.
Methods: A total of 676 HLA-A*0201–positive patients withunresectable stage III or IV melanoma, whose disease had progressedwhile they were receiving therapy for metastatic disease, wererandomly assigned, in a 3:1:1 ratio, to receive • ipilimumab plusgp100 (403 patients), • ipilimumab alone (137), or • gp100 alone(136). • Ipilimumab, at a dose of 3 mg per kilogram of body weight,was administered with or without gp100 every 3 weeks for upto four treatments (induction).
The median overall survival was 10.0 months among patientsreceiving ipilimumab plus gp100, as compared with 6.4 monthsamong patients receiving gp100 alone (hazard ratio for death,0.68; P<0.001). Grade 3 or 4 immune-relatedadverse events occurred in 10 to 15% of patients treated withipilimumab and in 3% treated with gp100 alone. ConclusionsIpilimumab, with or without a gp100 peptide vaccine,as compared with gp100 alone, improved overall survival in patientswith previously treated metastatic melanoma.
ClinCancerRes. 2009 Dec 1;15(23):7412-20. Epub 2009 Nov 24.Guidelinesfor the evaluationof immune therapyactivity in solidtumors: immune-relatedresponsecriteria.Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebbé C, Maio M, Binder M, Bohnsack O, Nichol G, Humphrey R, Hodi FS. The core novelty of the irRC (immune-related Response Criteria) is the incorporation of measurable new lesions into “total tumor burden” and comparison of this variable to baseline measurements
Caso Clinico 6 TA38INIZIO IPILIMUMAB AGOSTO 2006 Dicembre 2006 Febbraio 2008
15/12/06 23/06/07
Caso Clinico 6 TA38 Marzo 2010 Dicembre 2009
irAEs and their Treatment • The most common grade 3 and 4 class-related irAEs weredermatitis and colitis • Other serious but less common events includeduveitis, hepatitis and hypophysitis • The NCI Surgery Branch reported that, among 198 patients treated with Ipilimumab, 41 (21%) developed enterocolitis • The majority also presented diarrhea, fever and abdominal pain. • Histolpathology reports of bowel biopsies showed striking lymphocytic and neutophilic infiltration. • Five patients were refractory to corticosteroids and infliximab and underwent surgery for bowel perforation.
irAEs and their Treatment • Most irAEs were manageable with systemic steroids or other treatment. • Steroid treatmentdid not appear to affect antitumor efficacy The management of irAEs is different from that of other immunotherapies, such as IL-2 or IFN- α, or cytolitic chemotherapies: • Grade 1 and 2 toxicities generally resolve spontaneously. • Grade 3 or 4 toxicities require early interventionwith agents not typically used for AEs associated with antineoplastic therapy: the objective is to reduce the number of life-threatening outcomes (eg. corticosteroids to prevent diarrhea/colitis resulting in bowel perforation/colectomy).
irAEs and their Treatment • Guidelines for the management of Ipilimumab-associated diarrhea and hepatotoxicities have recently been published(Weber J. Oncologist 12(7), 864-872 (2007) • In 2007, NCI and ACS proposed some algorithms to manage colitis/diarrhea and hepatotoxicity that have been used in clinical trials(O'Day SJ, Cancer 110(12), 2614-2627 (2007).
CONCLUSIONS The Clinical Responses and the improved Survival in Patients with Metastatic Melanoma with anti-CTLA-4 Monoclonal Antibody are testing the effectiveness of Cancer Immunotherapy….