Download

1 / 23
230 likes | 375 Views
EUPHA Pre Conference Workshop migrant health. Health data collection on migrants and ethnic minorities in EU countries. A. Rosano, Regional Agency for Public Health, Rome, Italy L. Cacciani, Regional Agency for Public Health, Rome, Italy

E N D
EUPHA Pre Conference Workshop migrant health Health data collection on migrants and ethnic minorities in EU countries A. Rosano, Regional Agency for Public Health, Rome, Italy L. Cacciani, Regional Agency for Public Health, Rome, Italy S. Bruzzone, National Institute of Statistics, Rome, Italy N. Mignolli, National Institute of Statistics, Rome, Italy "This project is funded under the framework of Public Health Programme 2003-2008 of the European Commission (contract number 2005122)"
Background In Europe the number of migrants and ethnic minorities is increasing. Studies conducted in different countries have shown a worse health status among migrants compared to the general population, and a different access to health-care services. However, comparisons among EU countries are still lacking. In order to address this issue, a project on migrant health, Migrant and Ethnic Health Observatories (MEHO, http://www.meho.eu.com/), has been funded by the European Commission for 2007-2009.
Objective Within the MEHO project, the work package “Development of a set of comparable health indicators for migrants based on existing data in EU” has the main objective of taking a census of available information on migrants within health and socio-demographic databases in EU countries, and of building comparable health indicators.
Methods A questionnaire addressed to EU countries has been designed as the basic instrument to survey the most common criteria to define migrants or ethnic minorities, and to obtain a general overview of existing health and socio-demographic datasets in EU countries. Questions on definitions of migrants and on health and socio-demographic data sources have been included. The questionnaire has been piloted and then administered to members of the Statistical Programme Committee (SPC) network group, coordinated by EUROSTAT, that represents the official channel for statistical information.
The Questionnaire SECTION 1 - IMMIGRANT STATUS/ETHNICITY DEFINITIONS 1.1 - Is there an official definition for immigrants in your country? 1.2 - Are there other general definitions for immigrants in your country, different from the definition given above? 1.3 - Could you identify subgroups of people with a migrant/ethnic background that you would target as vulnerable in relation to health (e.g., ethnic minorities, refugees, roma people, immigrants exposed to occupational risks)?
The Questionnaire SECTION 2 - HEALTH DATA SOURCES General information on data sources 2.1 - Name of data source, with reference to form/questionnaire and acronym (English version) 2.2 - Background information 2.3 - Type of data source 2.4 - Minimum geographical level 2.5 – Coverage 2.6 - Population covered 2.7 – Periodicity 2.8 - Temporal availability 2.9 - Temporal comparability of data 2.10 - Data format
The Questionnaire SECTION 2 - HEALTH DATA SOURCES Information on immigrant/ethnic status 2.11 - Availability of immigrant/ethnic status information 2.12 - Temporal availability of immigrant/ethnic status information 2.13 - Possibility of retrieving immigrant/ethnic status information through record-linkage with available socio-demographic data sources 2.14 - Availability of identification variables to be used in record-linkage 2.15 - Availability of demographic and socioeconomic information 2.16 - Ethical/privacy/legal issues hampering accessibility to data source 2.17 - Data source owner or Institution/Organisation managing data 2.18 - Address of data source owner 2.19 - Name of contact person 2.20 - Address of contact person 2.21 - Documents available on this data source (e.g., publications, reports, websites or links)
The Questionnaire SECTION 3 - SOCIO-DEMOGRAPHIC DATA SOURCES General information on data sources 3.1 - Name of data source/Acronym (English version) 3.2 - Background information 3.3 - Type of data source 3.4 - Minimum geographical level 3.5 – Coverage 3.6 - Population covered 3.7 – Periodicity 3.8 - Temporal availability 3.9 - Temporal comparability of data 3.10 - Data format
The Questionnaire SECTION 3 - SOCIO-DEMOGRAPHIC DATA SOURCES Information on immigrant/ethnic status 3.11 - Availability of immigrant/ethnic status information 3.12 - Availability of linkage variables 3.13 - Availability of socioeconomic information 3.14 - Ethical/privacy/legal issues hampering accessibility to data source 3.15 - Data source owner or Institution/Organisation managing data 3.16 - Address of data source owner 3.17 - Name of contact person 3.18 - Address of contact person 3.19 - Documents available on this data source
Results • The questionnaires sent were returned by the due date (30/4/2008) by 20 countries out of 27: Austria, Belgium, Bulgaria, Cyprus, Czech Republic, Denmark, Finland, Germany, Greece, Ireland, Italy, Latvia, Lithuania, Malta, The Netherlands, Poland, Portugal, Romania, Slovenia, Sweden. • A second request was sent in June 2008 to non respondents ( France, UK, Spain, Estonia, Luxembourg, Hungary, Slovak Republic) with no success. • Preliminary findings confirm heterogeneity in availability of health and socio-demographic data.
Results Number of questionnaires by type
Results GENERAL SECTION AND DEFINITIONS • Two thirds of respondents stated to have an official definition for immigrants (Belgium, Bulgaria, Cyprus, Czech Republic, Denmark, Finland, Italy, Latvia, Lithuania, The Netherlands, Portugal, Romania, Slovenia, Sweden). • 10 out of the 17 respondent countries answered to have also different definitions. • Only six countries (Denmark, Finland, Italy, Latvia, Malta, The Netherlands) were able to identify subgroups of people with a migrant/ethnic background to be targeted as vulnerable.
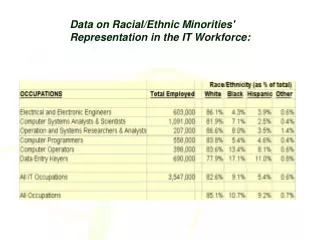
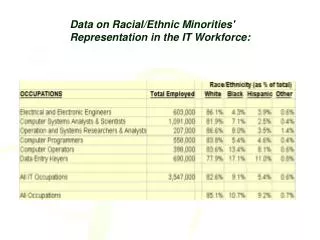
Results HEALTH SECTION • Two thirds of the countries responded on the type of available data (individual or aggregated). Among responding countries, the majority reported to have individual data (80%), with the exclusion of one source each for four countries: Austria, Belgium, Latvia and Poland. • The types of data sources are mainly hospital data, death registries, birth registries or disease registries. • The majority of the country data sources have information at municipal level (32%), 21 % at national level and 15% regional level. Other levels were reported in 15% of reported health sources, and 14% were not able to identify the geographical level.
Results HEALTH SECTION • For a few data sources (all those from Cyprus and Slovenia, Greece) the coverage (number of records) was not reported (10%), and 20% did not report the population covered. • Periodicity, and temporal availability and comparability were not reported in 20% of data sources. • Data were available in electronic format in 82% of data sources
Results HEALTH SECTION • Information on immigrant/ethnic status was reported as available in 81% of the health data sources, excluding two data sources from Malta, two from The Netherlands and three from Poland. Two thirds of respondents have information on the temporal availability of immigrant/ethnic status • In less than half of the health data sources (41%) it was possible to retrieve immigrant/ethnic status information through record-linkage with other socio-demographic data and 47% reported the variable to be used for the record linkage • Ethical/privacy/legal issues that may hamper accessibility to data source were reported in 73% of health data sources, whereas all the data sources from Austria and Germany have not such a limitation.
Results SOCIO-DEMOGRAPHIC SECTION SECTION • In 55% of the data sources it was possible to obtain information at the individual level with regard to demographic data (in 29% it was reported that information are at aggregated level and for 16 data sources we did not receive any answer). • The types of data source are mainly registries (general population and foreigner) (56% of the data sources) other than the census (22%) and other sources (22%). • The majority of the country data sources have information at municipal level (34%), 22% at regional level and 16% national level. Other levels were reported in 19% data sources, and 9% were not able to identify the geographical level
Results SOCIO-DEMOGRAPHIC SECTION SECTION • For all data sources the coverage (number of records) and the population covered was reported. • Periodicity, temporal availability and comparability were not reported in 25% of data sources. Data were available in electronic format in 84% of cases. • Information on immigrant/ethnic status was reported for 93% of the socio-economic data sources for responding countries (with the exclusion of one source from Sweden and one from Italy). • In more than half of the health data sources (55%) it was possible to retrieve immigrant/ethnic status information through record-linkage with other socio-demographic data and 47% reported the variable to be used for the record linkage • The ethical/privacy/legal issues that may hamper accessibility to data source were reported in 53% of data sources
Results Analysis of the 48 surveys with health data including information on immigrant/ethnic status through key characteristics of the surveys Characteristics % of positive answers • Availability of individual data 68.8% • Minimum geographical level (municipal) 56.3% • Population covered (total) 85.4% • Data format (electronic) 89.6% • Temporal availability of immigrant/ethnic 37.5% (at least 5 years/surveys) • Possibility of record linkage 37.5%
Discussion • The use of a standardised questionnaire, built within the framework of this large-scale European study on migrant health, is an important starting point to make a census of the existing health-care information related to migrants. • The choice to contact members of the SPC minimised non response due to the respondent burden, as SPC members are able to re-address the questionnaire to (or to indicate) the more appropriate respondent if necessary. • Nevertheless, some specific questions were not properly addressed and this implies an additional effort to reach the completeness of requested information.
Conclusion Out of the 59 health data sources censed in 20 EU countries, 48 include information on immigrant/ethnic status (81%). Almost all are available in electronic format. The first year of inclusion of information on immigrant/ethnic status varied from 1986 (Denmark) to 2005 (Germany). Previous studies reported “in most European countries there are few national or European surveys currently available to measure the health of migrants relative to the health of the native population”. (Mladoski, 2007) Now the situation seems to be improved. In 13 countries out of the 20 surveyed information on immigrant/ethnic status is available, such as in many data sources.
Conclusion Comparability is hampered by heterogeneity in the definition of immigrant/ethnic status, but also completeness and/errors in the registration of data of immigrants are key issues. Collection of comparable historical data is hence hardly feasible. Most surveys depend on a broad ‘social science’ definition of immigrant status, employing country of birth, parental country of birth and length of stay in the host country as indicators to identify this population. (Research note on Migration and Health in EU, Mladoski, LSE 2007)
Conclusion • Preliminary findings confirm heterogeneity in availability of health and socio-demographic data. • Availability of data on migrant health may vary among EU countries both as consequence of the development of the statistical system and because of differences in health policies. Because there are strong regional variations in the nature and size of the migrant population in Europe, it is not surprising that the amount of attention paid to migrant health issues varies greatly. (Good practice on health and migration in the EU, Lisbon 2007)
Future steps • Many studies and survey are now available on migrant health in EU. Additional effort should be devoted to summarise available information. • To propose / to use harmonisation criteria for future surveys. The European Union has recently issued a regulation (n. 862/2007) regarding community statistics on migration which is applicable to all member countries. It is based on the United Nations criterion, i.e. a period of residence of at least one year . "Disclaimer: The study has received funding from the European Commission under the Public Health Programme 2003-2008. However, the sole responsibility for the study lies with the author and the European Commission is not responsible for any use that may be made of the information contained therein."