Download
1 / 34
340 likes | 503 Views
Dive into bedside cognitive assessment instruments and their practical applications for older adults. Enhance your skills and explore various cognitive screening tools. Uncover areas of assessment, scoring methods, and executive functioning details.

E N D
Bedside cognitive assessment: instruments & applicability (In house Skill Development Program, 30 Nov to 5 Dec, 2015) Dr Rakesh Kumar Tripathi, M Phil, PhD Assistant Professor & Clinical Psychologist Department of Geriatric Mental Health King George’s Medical University Lucknow -226003 (India)
Bedside cognitive assessment: instruments & applicability Learning Objectives: • Cognitive assessment • Areas of cognitive assessment for elderly • Practical exposure to assess Cognitive functions • Basic skills for assessment • Cognitive screening tools from India
Cognitive Assessment of Older Adults Purpose of Bedside Assessment: • To screen the pt for probable diagnosis • To know differential diagnoses • For referral • Management/Rehabilitation • Improvement • Prognosis
Cognitive Assessment of Older Adults Areas of assessment • Cognition: • Orientation, • Attention & Concentration, • Calculation, • Memory, • Language, • Visuospatial function, • Praxis, • Executive function & social behaviour
Folstein et al. 1975 Scoring: 0- 4: Severe, 5-14: Mod. 15-19: Mild Dementia; 20-24: MCI, 25-28 Age related Cog Impairment, 29-30:Normal Normals can be expected to score > 25 However, even with > 25, if 0/3 or 1/3 for recent memory or problems with naming, repeating, writing or reading suggest focal deficits. It is most sensitive to disturbances which broadly effect function, it may miss subtle, focal problems.
International Psychogeriatrics (2009), 21:1, 123–128 C 2008 International Psychogeriatric Association Applicability of the Mini-mental State Examination (MMSE) and the Hindi Mental State Examination (HMSE) to the urban elderly in India: a pilot study ....................................................................................................... S. C. Tiwari, Rakesh Kumar Tripathi and Aditya Kumar Department of Geriatric Mental Health, C.S.M. Medical University (Uttar Pradesh), Lucknow, India Results: Either HMSE is screening more false negatives within the urban literate population or MMSE is screening more false positives within the illiterate population.
Indian Journal of Geriatric Mental Health, 7(2), 83-96, 2011. IAGMH/Intas Award 2011 at 3rd place. Development of an Education and Culture Fair Hindi Cognitive Screening Test (HCST) for the Elderly Population of India S. C. Tiwari and Rakesh Kumar Tripathi (2011) Department of Geriatric Mental Health C. S. M. Medical University, U P, Lucknow, India Sensitivity: 0.93 Specificity: 0.96 Reliability (r): -0.87 with Brief Cognitive Rating Scale (Reisberg & Ferris, 1988)
Attention & Concentration • Spelling of a 5 word backwards e.g. ‘World’ or ‘Right’ • 100-Serial 7’s or 20-3’s • Vigilance test: "I am going to say a long series of letters. Whenever you hear the letter A, indicate by tapping the desk.“ Speak a random series of letters at a normal rate with A occurring regularly and sometimes repeating as in the following example: • “K T B A O S A W I E A A G H C A T A A A E ...” • Digit span Localisation: Normal attention and concentration requires optimal interaction between the reticular formation, thalamus and neocortex
Memory-not a Unitary Process Sensory Memory Short term memory Long term memory Recent memory Remote memory Working memory Episodic memory Semantic memory
Working Memory • Ability to temporarily maintain and manipulate information that one needs to keep on-line • Divided into components that process phonologic information (e.g. phone number in head) and components process visual (mentally following a route) with central executive • Poor working memory leads to faulty encoding • Overlap with attention • Bedside task- digit span test
Semantic Memory Localisation
Localisation • In more than 98% of right handers the peri-sylvian language areas of the left hemisphere are responsible for language processing. • This includes Wernicke’s area, the arcuatefasciculus,Broca’s area and other associated cortical areas. • The right hemisphere is involved in other aspects of language such as humour, metaphor and determining the emotional state of the speaker.
Executive Function A complex set of cognitive abilities that are involved in planning and multitasking Frontal cortices Localisation • The frontal cortices are involved in executive functioning and it connects closely with subcortical structures. These connections form loops projecting from the frontal cortex to the striatum, globuspallidus, thalamus and back to the frontal cortex. • Lesioning in any part of this circuit will result in deficits that are indistinguishable from a frontal cortical injury. The anterior cingulate has many connections with the frontal lobes and are also involved in executive functioning. Subcortical structures Frontal cortex Striatum Globus pallidus Thalamus Anterior cingulate
Friends! Please follow the instructions and do mistakes to learn scoring • Draw a clock face (large circle) • mark the hours (numbers in the circle) • draw a time 10 past 11
Bedside Cognitive Assessment of Older Adults Clock drawing Test Score≥ 3: Cognitive deficit
Basic communication Skill for Assessment • Calm, reassuring tone of voice • Explain what you are going to do prior to moving into the patient’s personal space to implement care/assessment • Use a non-threating posture • Do not approach the patient from behind • Touch and care should be in a respectful, careful and unhurried manner • Use short words and simple sentences • Ask one question at a time • Don’t ask ‘why’ • Give adequate time for response • Repeat questions and instructions if necessary • Speak slowly and clearly • Use of aids (hearing, vision, physical) by the patient Sing I & Tripathi SM (2013). Management of BPSD. In Tiwari SC & Pandey NM (eds.) Geriatric Mental Health at a Glance ,pp 81-95. Ahuja Publishing House , New Delhi , India.
Psychological Assessment of Older Adults Screening • Mini Mental State Examination (MMSE) (Folstein et al. 1975) • Hindi Mental State Examination (HMSE) (Ganguli et al. 1995) • Hindi Cognitive Screening Test (Tiwari and Tripathi, 2011) • St. Louis University Mental State (SLUMS) Exm. (JE Morley, 2000) • Clock Drawing Test (CDT) (Shulman et al. 1993) • Bender Gestalt Test (BGT) (Lauretta Bender, 1938) • Hachinski Ischemic Scale (1975) • 7 Minute Neurocognitive Screening Battery (Solomon et al. 1998) • Short Portable Mental State Questionnaire (E. Pfieffer, 1975) • Community Screening Instrument for Dementia (Hall et al. 1993) • Brief Cognitive Rating Scale (BCRS) (Reisberg and Ferris, 1998) • Functional Assessment Staging (FAST) (Reisberg, 1988) • Global Deterioration Scale (GDS) (Reisberg, 1988) • Cognistat(Northern California Neurobehavioural Group, 1995 ) • Indian adaptation of Cognistat(Gupta and Kumar, 2009) • Addenbrooke’s Cognitive Examination (2005 to 2012) • Montreal Cognitive Assessment (Nasreddine, 1996)
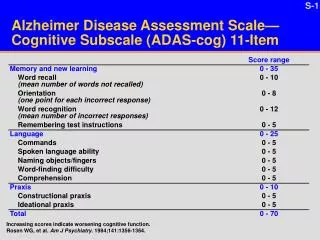
Bedside Cognitive Assessment of Older Adults • St. Louis University Mental State Examination (SLUMS Exam.) Morley JE, 2000 • It is a simple 11 items tool • * Mild Neurocognitive Disorder • Takes about 5-10 minutes in administration • SLUMS is more sensitive in detecting MCI and dementia than Mini Mental • State Examination
Bedside Cognitive Assessment of Older Adults Hachinski Ischemic Scale (1975) Scoring 0-4: Alzheimer's Dementia; 5-6: diagnosis unclear; 7 or more : Vascular Dementia
Montreal Cognitive Assessment (Nasreddine, 1996) 10-15 minutes •Score / 30 •Better sensitivity than MMSE for MCI •Needs more clarity about cutoff scores? •Mean score of normal population 26-27 •Cutoff at 26 gives high sensitivity but low specificity •Suggested guide is <22 for MCI, AD < 17
Cognitive screening tools from India (contd.) Adaptation Community based Tiwari & Tripathi, 2011 Like MMSE 300 60 &+ In Progress Bias Free KGMU,Lucknow, UP Hindi Yes
King George’s Medical University, Lucknow, U.P., INDIA Contact: R K Tripathi rastripathi@gmail.com 91+9454202905 Thank you