Download
1 / 1
10 likes | 143 Views
The Impact of Mental Health Conditions on Maintenance of Risk Factor Control in Diabetic Patients After Discharge from a Cardiovascular Risk Reduction Clinic Lisa B. Cohen, Pharm.D . 1,2 , Tracey H. Taveira Pharm.D . 1,2 , Wen-Chih Wu, MD 1,3 , Paul Pirraglia, MD, MPH 1,3

E N D
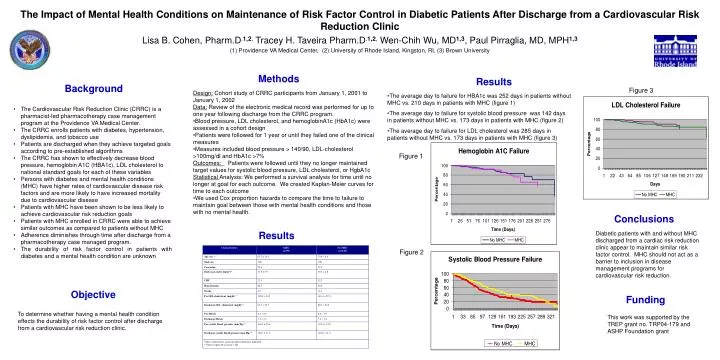
The Impact of Mental Health Conditions on Maintenance of Risk Factor Control in Diabetic Patients After Discharge from a Cardiovascular Risk Reduction Clinic Lisa B. Cohen, Pharm.D.1,2, Tracey H. Taveira Pharm.D.1,2, Wen-Chih Wu, MD1,3, Paul Pirraglia, MD, MPH1,3 (1) Providence VA Medical Center, (2) University of Rhode Island, Kingston, RI, (3) Brown University Results Methods Background Figure 3 • Design: Cohort study of CRRC participants from January 1, 2001 to January 1, 2002 • Data: Review of the electronic medical record was performed for up to one year following discharge from the CRRC program. • Blood pressure, LDL cholesterol, and hemoglobinA1c (HbA1c) were assessed in a cohort design • Patients were followed for 1 year or until they failed one of the clinical measures • Measures included blood pressure > 140/90, LDL-cholesterol >100mg/dl and HbA1c >7% • Outcomes: Patients were followed until they no longer maintained target values for systolic blood pressure, LDL cholesterol, or HgbA1c • Statistical Analysis: We performed a survival analysis for time until no longer at goal for each outcome. We created Kaplan-Meier curves for time to each outcome • We used Cox proportion hazards to compare the time to failure to maintain goal between those with mental health conditions and those with no mental health. • The average day to failure for HBA1c was 252 days in patients without MHC vs. 210 days in patients with MHC (figure 1) • The average day to failure for systolic blood pressure was 142 days in patients without MHC vs. 173 days in patients with MHC (figure 2) • The average day to failure for LDL cholesterol was 285 days in patients without MHC vs. 173 days in patients with MHC (figure 3) • The Cardiovascular Risk Reduction Clinic (CRRC) is a pharmacist-led pharmacotherapy case management program at the Providence VA Medical Center. • The CRRC enrolls patients with diabetes, hypertension, dyslipidemia, and tobacco use • Patients are discharged when they achieve targeted goals according to pre-established algorithms • The CRRC has shown to effectively decrease blood pressure, hemoglobin A1C (HBA1c), LDL cholesterol to national standard goals for each of these variables • Persons with diabetes and mental health conditions (MHC) have higher rates of cardiovascular disease risk factors and are more likely to have increased mortality due to cardiovascular disease • Patients with MHC have been shown to be less likely to achieve cardiovascular risk reduction goals • Patients with MHC enrolled in CRRC were able to achieve similar outcomes as compared to patients without MHC • Adherence diminishes through time after discharge from a pharmacotherapy case managed program. • The durability of risk factor control in patients with diabetes and a mental health condition are unknown Figure 1 Conclusions Results Diabetic patients with and without MHC discharged from a cardiac risk reduction clinic appear to maintain similar risk factor control. MHC should not act as a barrier to inclusion in disease management programs for cardiovascular risk reduction. Figure 2 Objective Funding To determine whether having a mental health condition effects the durability of risk factor control after discharge from a cardiovascular risk reduction clinic. This work was supported by the TREP grant no. TRP04-179 and ASHP Foundation grant






















