Download
1 / 20
200 likes | 414 Views
Physiology of the Adrenal Glands and Pancreas 1/11. Review of the autonomic nervous system (please review CH 15 on your own) What are the two faces of the adrenal gland? Cortex and Medulla What are the Hormones of Cortex? What are the Hormones of Medulla?

E N D
Physiology of the Adrenal Glands and Pancreas 1/11 • Review of the autonomic nervous system (please review CH 15 on your own) • What are the two faces of the adrenal gland? Cortex and Medulla • What are the Hormones of Cortex? • What are the Hormones of Medulla? • What are some pharmacological applications? • What is the function of the pancreas? • What is are the two types of diabetes mellitus?
Next Week we will have 5 pt pre-lab quizzes EXAMPLE Lab 2: 5 point pre-lab quiz- Choose the best answer (No Quiz This Week) 1) True or False: We will measure the ventricular volume of the heart in today’s lab. 2) Which of the following is a preserved heart we will study in today’s laboratory activity? a) Pig b) Cow c) Sheep d) Dog e) Plastic model 3) True or False: The pig heart is quite different from the human heart anatomically. 4) We will NOT identify arteries and veins using which of the following? a) Preserved Cat b) Cadaver c) Torso model d) Microscope e) All the above will be used 5) True or False: The structures of the electrical conduction system are easily identified on the models, preserved hearts and fresh hearts, any of which may be used for the lab exam.
What is the function of the autonomic nervous system? (Please review the Autonomic Nervous System CH 15) Two ANS branches: the parasympathetic NS (PNS) used during relaxation and the sympathetic NS (SNS) used during stress Parasympathetic NS: prepares body for functions that occur during the relaxed state (i.e. after a meal). Effects limited to cell at synaptic ending Acetylcholine (ACH) uses nicotinic then muscarinic receptors for ACH which is RAPIDLY destroyed at synapse Time of effect is very brief (msec) Sympathetic NS: Prepares the body to FIGHT or Run Away! Two catecholamines: epinephrine/norepinephrine released at a synapse NT or released into blood (endocrine) Catecholamines are destroyed much more slowly than ACH Why is time to effect longer? (msec, seconds, minutes or more) VIP: SNS can also turn off the PNS!
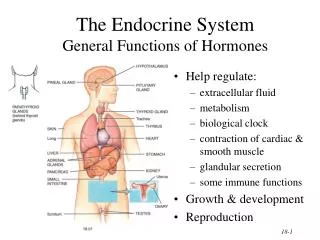
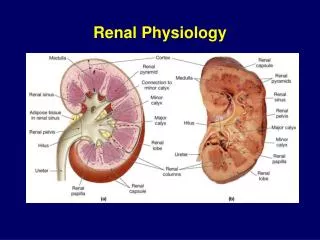
The adrenal glands are located superior to the kidneys and help manage STRESS. The adrenal gland has two parts: an outer cortex makes steroid-based hormones and an inner medulla makes water soluble catecholamines (SNS). All these endocrine hormones are delivered to body by the blood stream!
Why is it so important that the medulla be so vascular in terms of the time needed to generate a physiological response to EPI and NE? The cortical regions take more time to produce their steroids and secrete their hormones slightly less rapidly. What would happen to your stress response time if you had poor adrenal gland circulation? EPI/NE DHEA/Sex Steroids GlucocorticoidsMineralocorticoids What hormones are produced in what parts of adrenal gland?
The Fight or Flight response works because exocytosis dumps Epinephrine and Norepinephrine into the blood or into a synapse. What are the structures of EPI and NE? How do drugs that look like these catecholamines work?
NE and EPI specifically bind to adrenergic receptors! How do you fine-tune adrenergic effects in the body? Are all adrenergic receptors alike? There are at least 5 different types of adrenergic receptor: each receptor gives a different effect! • Heart: ↑Force of Contraction: Beta 1 (+ adenylyl cyclase) • Lung: ↑Bronchodilation: Beta 2 (+ adenylyl cyclase) • Fat: ↑Energy release via Beta 3 (+ adenylyl cyclase) • Vasoconstriction/↑Heart Rate: Alpha 1 (+phospholipase C) • Inhibition (IPSP:↑intracellular K+): Alpha 2(-adenylyl cyclase) • Important: Can you still name a function for each receptor subtype? (Good T.Q.)
Why can a single hormone affect different cells very differently? Why can the effect of a hormone on a cell change over time? 1) What if a one heart cell has many alpha-1 receptors and another has very few? Will all heart cells and people respond the same? 2) What if the cells of the lung begin to express fewer beta-2 receptors? Will your albuterol inhaler still prevent asthma? 3) How does each mechanism support a different part of fight or flight? 4) Why might it be useful to “tailor” a response (drug) so just one receptor type is activated?
THE ADRENAL MEDULLA CONTAINS A LARGE NUMBER OF CELLS THAT RELEASE EPI/NE INTO THE BLOOD (INSTEAD OF A SYNAPSE) so the catecholamines are delivered to the entire body! • Sympathetic Nervous System has two ways to deliver info: • 1) Preganglionic axons innervate postganglionic cell that releases EPI/NE into a specific synapse on a specific target cell in a specific tissue. • 2) Preganglionic axons innervate postganglionic cells of the adrenal medulla that store EPI/NE in vesicles. Exocytosis is used to secrete NE and EPI into interstitial fluids followed by diffusion through fenestrations to blood. Epi/Ne diffuses from blood through interstitium to target adrenergic receptors located on platelets, endothelial cells, or cells in tissues (i.e. heart)). • THESE ARE TWO “REDUNDANT” DELIVERY METHODS! • Why is redundancy important to cardiac function if you have a transplanted heart! • Adrenergic receptors on target cells are very selective and only accept EPI or NE!
Many common drugs have their effect because they look like (mimic) the catecholamines. • Allergies: Alpha-1 is used to dry up mucus membranes during stress, therefore you take phenylephrine as a decongestant! • High Blood Pressure: Alpha-1 increases heart rate and causes vasoconstriction. • You may take the drug “Prazosin” to block the receptor so EPI/NE cannot activate PL-C. • High Blood Pressure: Beta-1 increases the force of contraction and can cause high blood pressure. • The drug “Atenolol” fills the Beta-1 receptor so EPI/NE cannot activate adenyl-cyclase • Asthma: Beta-2 promotes promotes bronchodilation • The drug “Albuterol” looks like EPI to preferenentially to Beta-2 receptors and turns Adenylyl cyclase on in only these cells (bronchodilationyou can breath again) • CNS Inhibition: Yohimbine prevents Alpha-2 receptor activation, changing membrane potential of target cells. (Sex Begins Again)
Because steroids are lipid-based it is difficult to store them. As a result the cells of the adrenal cortex produce and secrete their steroid hormones when stimulated. Production takes time. Therefore, the steroid response time is slower than for catecholamines. EPI/NE DHEA/Sex Steroids GlucocorticoidsMineralocorticoids What hormones are produced in what parts of adrenal gland?
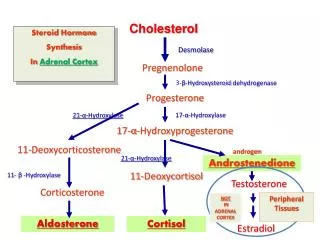
THE ADRENAL CORTEX SECRETES GLUCOCORTICOIDS, MINERALOCORTICOIDS AND STEROIDS INTO THE BLOOD. The 3 Cortical Layers of adrenal cortex are distinguished by their secretions of cholesterol-based endocrine hormones: • 1) Inner-Zona Reticularis: Anabolic and Sex Steroids • Creates a pre-hormone called Dehydroepandrosterone (DHEA) for production of testosterone/estradiol • Changes muscle development/personality • Most testosterone/estradiol produced in gonads • 2) Middle-Zona Fascicularis:Glucocorticoids- Cortisol • Change carbohydrate metabolism= +blood glucose • Catabolism of glycogen and protein • Suppression of Immune system and Inflammation • 3) Outer-Zona Glomerulosa:Mineralocorticoids- Aldosterone • Change sodium reabsorption/ +blood pressure
The adrenal cortex handles stress primarily by making cortisol , aldosterone, and DHEA which becomes testosterone and its product estradiol. Most DHEA is converted in the gonads. DHEA Prednisone and Dexamethasone are drugs that look like cortisol and have anti-inflammatory effects in the body just like cortisol.
What are the stages of stress and adaptation to stress? What is our health outcome if we are at ant one stage? • Stage 1: The Alarm Reaction • Stage 2: The Stage of Resistance • Stage 3: The Stage of Exhaustion • How does this apply to you when a mugger jumps from around a corner? • How does this apply to a soldier who has been in the field under fire for two months and come home on leave? • How does this apply to a loved one who is finally succumbing to cancer? • Why is it clinically important to consider the stage of stress that a person is experiencing?
THE PANCREAS SERVES AS BOTH AN ENDOCRINE and an EXOCRINE GLAND. IT RESPONDS TO THE GLUCOSE NEEDS OF THE BODY AND ITS FEEDING STATUS. • Exocrine secretions include digestive enzymes sent to duodenum…more next week • 3 Endocrine SecretionsInsulin Glucagon Somatostatin Islet of Langerhans: Beta Cells Alpha Cells Delta cells • Three Levels of Importance: • #1) Insulin: Universal Well-Fed signal>>Tyrosine Kinase Stimulates glucose uptake into cells as well as TG/glycogen/protein synthesis>>GROWTH • #2) Glucagon: Universal Starvation signal>>++cAMP Stimulates Protein,TG and Glycogen breakdown • #3) Somatostatin: released following feeding and inhibits BOTH glucagon and insulin releaseFeed Back!
Insulin Glucagon Somatostatin Digestive Enzymes and Bicarbonate
Beta Cell Insulin production and release is tightly regulated! Only a tiny part of the original pro-hormone is used to make the active hormone! The active hormone (insulin) is stored in secretory vesicles until release (exocytosis) is initiated by a calcium influx into the cell, this permits insulin secretion out of the cell to blood. Disulfide bonds between two cysteines in peptide sequence ACTIVE HORMONE Inactive Hormone or Zymogen
Insulin creates its effect by stimulating a Tyrosine Kinase.
There are three types of diabetes mellitus that are all characterized by pathogenically high blood glucose. Diabetes is the epidemic of our generation! MN and WI counties, within 25 miles of Winona State University based on 2008 Census data and the national Type 2 Diabetes estimate of 8.3% affliction. (CDC 2010). • Type I or Juvenile onset: Characterized by a lack of (or insufficient) insulin secretion after a meal (no beta cells) • Type II or Adult Onset: Characterized by the inability of cells in the body to response to insulin released from the pancreas. Insulin produced but does not function properly at target cells, eventually results in failure of beta-cells and insulin dependence • Gestational Diabetes: Characterized by a transitory insulin resistance during pregnancy. Abberation of an intent by mom’s endocrine system so save nutrients for the fetus (poorly understood etiology) • These three diseases are very different and cause very different problems.
Current criteria for the diagnosis of diabetesADA 2011 Standard of Care, Diabetes Care, 2011:34, S4-S10 Any One of Following Defines Person as Being Clinically Diabetic • Hemoglobin A1c Glycosylation Value: A1C 6.5%- measures long-term glycemic control. • Fasting plasma glucose (FPG) of 126 mg/dl (7.0 mmol/l) or more with no caloric intake for at least 8 hours • 2-hour plasma glucose of 200 mg/dl (11.1 mmol/l) or more during an oral glucose tolerance test (OGTT) with load of 75 glucose in water • Classic symptoms of hyperglycemia or hyperglycemic crisis, and random plasma glucose of 200 mg/dl (11.1 mmol/l) or more • In the absence of unequivocal hyperglycemia, result should be confirmed by repeat testing. • Testing for diabetes in asymptomatic (means one need not be aware of having disease symptoms-potentially silent)