Download
1 / 34
480 likes | 1.92k Views
Salivary Glands Tumors A short overview. Dr. Med. Ibrahim K. Lada‘a ENT-specialist 2009 Ramallah. benigne about 70% predominantly in the parotid glands Swelling without symptoms Surgery is the standard therapy. malignant Very low Incidence

E N D
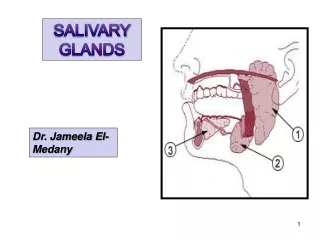
Salivary Glands TumorsA short overview Dr. Med. Ibrahim K. Lada‘a ENT-specialist 2009 Ramallah
benigne about 70% predominantly in the parotid glands Swelling without symptoms Surgery is the standard therapy malignant Very low Incidence Predominantly in the small salivary glands swelling with Malignant symptoms modified surgical therapy radiation therapy Salivary Glands Tumors
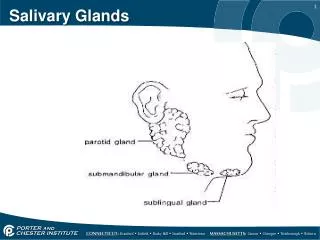
Salivary glands tumors • 2% of all Tumors • Gl. Parotidea: 80% • 70% Benigne • 30% Malignant • Gl. Submandibularis: 10% • 50% Benigne • 40% Malignant • small salivary glands(600): 5% • 70% Malignant • Gl. Sublingualis: 1%
Benigne Epithelial Pleomorphic Adenoma 45% Cystadenoma (Warthin tumor) 15% monomorph Adenomas 5% (Basalcell, Onkocytoma, Canalicular) Mesenchymal Hemangioma/Lymphangioma 2% Lipoma 2% others (Neurofibrom) 1% % to all Salivary glands tumors Malignant Epithelial Mucoepidermoid carcinomas 5% Carc. ex pleiomorphic adenoma 5% Cystadeno carcinoma 3% Adenocarcinoma 3% Undifferenciated carcinoma 3% Acinuscell carcinoma 2-3% Squamousepithelium carcinom 2% Non-epithelial Lymphomas 1-2 % Sarkoma < 1% others < 1% Salivary glands tumors
Pleomorphic Adenoma • Synonym: benign salivary gland mixed tumor • Microscopy: • epithelial elements in a mixed matrix • epithelial • Mucoid • Chondromatös • Hyalin • Macroscopy • capsulated • Even borderd o. lobbed
Pleomorphic Adenomaclinic and epidemiology • Most frequent Adenoma of the Salivary glands • Gl. Parotidea 85% • Gl. Submandibularis 5% • Gl. Sublingualis & small Salaivary glands 10% • W>M • 50-60 age • Malignant Transformation 3-5% (rises in case of recurrent tumor or size of tumor) • grows very slow • painless • Mostly unileteral
Pleomorphic AdenomaDiagnostic • Medical history • Inspection (special case: Eisbergtumor) • Palpation • mobile • Firm, elastic • Facial nerve control
Pleomorphic AdenomaDiagnostic • B- Mode Sonography: • even o. lobed borders • cystical parts • low echo • Low perfusion • Fine needle puncture • Different opinions • Frozen section
Pleomorphic AdenomaDiagnostics • CT or MRI • T2 T1 >>>>> Kontrast
Pleomorphic AdenomaTherapy • always Surgical • laterofacial parotidectomy (in sano resection) • keep tumor capsula intact!!!! • keep facial nerv alive (Facial nerve Monitoring) • If necessary total parotidectomy
Pleomorphic AdenomaPrognosis • good • excision with intact Capsula = no Residual • Capsula damage!: multilocal metastasis, surgical resektion very difficult with higher risk of facial nerv palsy • Don‘t wait too long • Malignant transformation risk • Surgical difficulty rises • Evtl. facial nerve palsy
Zystadenolymphoma • Synonym: Warthin Tumor • Possibility of viral Association • Epidemiology: • Second common Tumor of Gl. Parotis • 5:1 (M/W) • 10% bilateral, 10% multifokal • Age of 60 and up • Clinic: • Indolent Swelling at Parotisunderpole (Arcus mandibulae) • No malignant symptoms
CystadenolymphomaDiagnostic • medical history (months) • Inspection • Palpation • Sono: one or more Cystic structures • FNB: Hilft i.d.R. nicht weiter • CT/MRI • DD: 1) Lymphoma 2) Lymphoepithelialecysts
Therapy pericapsular excison Capsula close preparation very Slow growth Prognosis barely malignant transformation barely recurrent Cystadenolymphoma
Made up of blood vessels sometimes with intramural calcification rare < 2 % mainly at Kids and teenagers Blaufärbung unter der Haut, die durch Wegstreichen zunächst verschwindet, um kurz danach wieder aufzutauchen Therapy: surgical extirpation cm 1 2 3 4 6 5 Benign Parotid Tumors -Hemangiomas: short overview-
Salivary gland carcinomas Epidemiology • Incidence < 1: 100.000 • Percentage of malignant salivary gland tumors under all neoplasia • small SG: 70-80% • Gl. SL 50% • Gl. SM 35-50% • Gl. Parotis 20-30% • 50-60 age Clinical-Epidemiological Data of Pat. with Salivary gland carcinomas from TRM (tumor register Munich) 1978-2003
Salivary gland carcinomas atiologie & Risik factors • Almost unknown • Radiation exposition (25 years latency) • Genetic Aberrations (spez.) • Genetic Predispositoin (Breast & skin cancer) • Alcohol, cigarettes, nicel, Chrom, Asbest????
Salivary gland carcinomas Malignancy criteria • Skin infiltration • Lymph node Metastasis • Facial palsy • 46/378 malignant • 0/1750 benigne (Enroth et. al) • fast growing • Only at 8% (malignant tumors) • 2% at benigne tumors • pain • Painless swelling is the most common Leading symptom 56% • classical symptoms of Malignancy are not representativ. because 65-80% of the malignant tumors are clinically manifested as a singular node without Symptoms
Salivary gland carcinomas • challenging Diagnostic and Therapy • various histological Varietys • Different clinical history • anatomically close to the Facial nerve • low Incidence
Salivary gland carcinomasDiagnostics Obligatory: • clinical history • Inspection und palpation • solid, painless vs. painfull, fixed • clinical Function of N. facialis • Ultrasound of the parotid region and neck • Topography ( up to 100% Sensitivity) • Almost no differentiation • Postsurgical control
Salivary gland carcinomasDiagnostics • In some cases is CT or MRI usefull: • CT or MRI • medial Parotid lobe • Parapharyngeal space • CT: • Exclusion of bone infiltration • MRI: • Exclusion of soft tissue infiltration (N. Facialis) • Local recurrence • Carcinoma Differentiation (Gadolinium with T1 sequences) • PET: (Glucosestoffwechsel) • Differntiating between Scar tissue & Recurrence (very expensive)
Salivary gland carcinomassurgical therapy • Complete tumor excision • Eventually neckdissection from Level I-V • Maintainance of the N. Facialis/ Reconstruction in same session
When to perform ND Salivary Gland Cancer N+ Neck N0 Neck High Grade Carcinoma T1 - T4 Low Grade Carcinoma T2 - T4 Low Grade Carcinoma T1 Neck Dissection Level I - V Neck Dissection Level I - III Neck Dissection Not Required
Radiotherapy • Compatible for all histological entitys exepct for: • High differntiated Mucoepidermoid carcinomas • Azinus cell carcinoma • Primary Radiotherapy: • inoperable Tumors • Recurrence tumors with palliativ case
When to performPostsurgicalradiation ? • Recurrence • R1- or R2- excision • Infiltration of neighboring structures • N+ • T3, T4-Malignomen generell, • High-grade Malignomas • Adenoidcystic carcinoma
5 year survival after combined therapy • combination of surgery & radiotherapy can improve the 5-year survival significantly! combined versussurgeryalone • Stage T3,T4: 51% vs. 10% • N+: 49% vs. 19% • High-grade Malignomas: 57% vs. 28%
Adenoidcystic carcinomashort overview • Synonyma: cylindroma • 8% of all salivary gland carcinomas • mainly in small salaivary glands (palate) • boneinfiltration • Perineural + Perivascular invasion • Metastasis: Hematogenic 40-60%, Lymphogen 8% • Slow growth –(some cases fulminant growth) • Radiotherapy resistance • 5-year survival: 75%
carcinoma ex pleomorphic Adenoma • 7% of all salivary gland carcinoma • 8% of pleomorph adenoma degenerate to carcinoma • mainly Gl. Parotis • Risk factors: • Local recurrence of pleomorphic adenomas • Waiting over 10 years for excision
Take HomeMessage • In general • The smaller the gland the higher the chance of a carcinoma • Diagnosis and Therapy very simillar in all cases • Mainly elderly >50 (Exception: Hämangioma(teenagers) and Mucoepidermoid carcinomas <50)
Take HomeMessage • Benign Tumors • Pleomorphic Adenoma • Candegenerate to malignantcarcinoma • Completetumorexcisionwithintactcapsula
Take HomeMessage • Malignant Tumors • Mucoepidermoidcarcinoma : chestX-ray • Adenocysticcarcinoma: radiotherapyresistant • Malignant Symptoms (facialpalsy,pain, skininfiltration, metastasis,fastgrowing) arenotobligatorysince 65-80% have no malignantsymptoms • comb. of Surgery + Raditherapyimproves 5-year survivalsignificantly
Saliva is not only associated with foodIn fact some unusual uses of saliva are to preserve social status among lamasHowever what is spat by the lama is not actually saliva, but rather a digestive acid, that is both green and has a foul odor.Rest assured though, that it is easily washable, just in case you have an unfriendly encounter with a lama