Download
1 / 14
150 likes | 619 Views
“KEYHOLE” CRANIOTOMY. EARLIER MORE EXTENSIVE. Ultrasound Guided Aspiration +/- Thrombolytic Agent. DECOMPRESSIVE CRANIECTOMY FOR ICH. Decompressive Craniectomy +/- evacuation of ICH Improve ICP, hemodynamics and metabolic parameters Murthy et al: Neurocrit. Care 2005

E N D
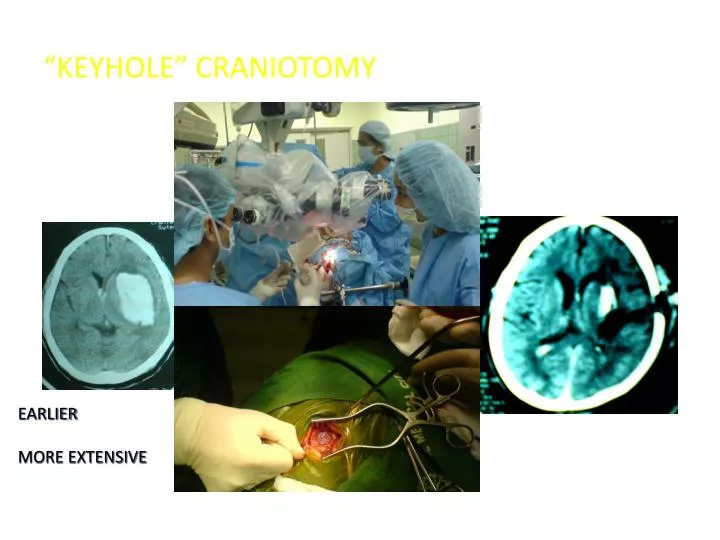
“KEYHOLE” CRANIOTOMY EARLIER MORE EXTENSIVE
DECOMPRESSIVE CRANIECTOMY FOR ICH Decompressive Craniectomy +/- evacuation of ICH Improve ICP, hemodynamics and metabolic parameters Murthy et al: Neurocrit. Care 2005 12 pxs, GCS 5-8, 92% survived 54.5% good outcome Schaller et al; Brain Res 2003 May be better with evacuation of ICH? Dierssen et al ACTA Neurochirg 1983
Decompressive Craniectomy Most minimally invasive?
OCCLUSIVE STROKE Intracranial Stenosis Intraarterial Thrombolysis Angioplasty with stenting EC-IC Bypass for chronic ischemia Predicted to increase in numbers Need to retrain the neurosurgeons Indications Skills
62/f Neurologist L MCA Occlusion INTRAARTERIAL THROMBOLYSIS (rTPA) on the 6th hour
MALIGNANT MCA INFARCTION DECOMPRESSIVE CRANIECTOMY
DECOMPRESSIVE HEMICRANIECTOMY ICP PtiO2 EFFECT ON ICP AND PtiO2
Decompressive Craniectomy Increasing in acceptance and usage PGH: Site of RCT Only one ongoing as of now Factors to increase good outcome Younger (55 y) Earlier (<48 hrs) Non fulminant course /Dilemna of doing it too early or too late
Decompressive Craniectomy HeMMI: Hemicraniectomy for Malignant Middle Cerebral Artery Infarcts. Jamora,R, Chua, A., Collantes, E., Manila/Philippines Year started 2004 Study size actual 26 (12 Medical) Study size planned 56 Age 15-65 Timing of surgery <72 hrs
Decompressive Craniectomy RCT s in Hemicraniectomy Improved survival Is this enough? For most families it is