Download
1 / 65
650 likes | 674 Views
Learn about the cardiac cycle phases, ventricular action potential, ECG interpretation, lead systems, normal sinus rhythm, different heart block types, and the pathologies leading to arrhythmias. Get insights into bradycardia, tachycardia, PVC, atrial fibrillation, ventricular tachycardia, and more.

E N D
Heart Rate and ArrhythmiaBasics Kevin Formes D.O. July 27, 2004
Cardiac Cycle • Phase 0: Rapid depolarization • Sodium moves rapidly into the cell • Calcium moves slowly into the cell • Phase 1: Early repolarization • Sodium channels close • Phase 2: Plateau • Calcium continues to flow in • Potassium continues to flow out • Phase 3: Rapid repolarization • Calcium channels close • Potassium flows out rapidly • Active transport Na/k pump • Phase 4: Resting • Cell membrane is impermeable to sodium • Potassium moves out
0.2 sec Ventricular Action Potential & ECG QRS T
Heart Physiology: Sequence of Excitation Figure 17.14a
Heart Physiology: Sequence of Excitation • Sinoatrial (SA) node generates impulses about 75 times/minute • Atrioventricular (AV) node delays the impulse approximately 0.1 second • Impulse passes from atria to ventricles via the atrioventricular bundle (bundle of His)
Electrocardiography • Electrical activity is recorded by electrocardiogram (ECG) • P wave corresponds to depolarization of atrium • QRS complex corresponds to ventricular depolarization • T wave corresponds to ventricular repolarization • Atrial repolarization record is masked by the larger QRS complex
The 8-Step method • Determine the rhythm • Determine the rate • Determine the axis • Evaluate the p wave • Determine the duration PR interval • Determine the duration of QRS complex • Determine the duration of QT interval • Evaluate ST segment and T wave
Methods To Determine Rate • Distance between the R-R interval (300/#large blocks) • 1 large block 300 • 2 large blocks 150 • 3 large blocks 100 • 4 large blocks 75 • 5 large blocks 60 • 6 large blocks 50
Lead Systems: • In 1902, Willem Einthoven recorded the first EKG. He determined that the heart lies at the center of the electrical field determined by the axis of three standard “Limb” electrodes. • Different “leads” or views of the electrical patterns produced were obtained by electrodes placed on the Left Arm, Right Arm, and Left Leg.
Electrocardiogram (ECG):Electrical Activity of the Heart • Einthoven's triangle • P-Wave – atria • QRS- wave – ventricles • T-wave – repolarization Figure 14-20: Einthoven’s triangle
Cardiac Axis by different Leads Carr and Brown Figure 8-2
Pathological Conditions Mean Electrical Axis (mark changes in current flow) Left Axis Deviation (hypertrophy of left ventricle) 1. Hypertension (muscle mass on left side of heart) 2. Aortic Valvular stenosis 3. Aortic Valvular regurgitation 4. Several congenital heart conditions Right Axis Deviation 1. Hypertrophy of right ventricle (pulmonary stenosis) 2. Tetralogy of Fallot (congenital right to left shunt )
Precordial (chest) Leads R L V6 - V5 V4 V3 V2 V1
Electrocardiogram (ECG):Electrical Activity of the Heart ≤100 msec 120-200 msec ≤450 msec
Normal Sinus Rhythm • Sinus node is the pacemaker, firing at a regular rate of 60 - 100 bpm. Each beat is conducted normally through to the ventricles • One P wave for each QRS • PRI: .12-.20 seconds and constant • QRS: .04 to .1 seconds
Bradycardia Tachycardia 1st degree AV block 2nd degree AV block 3rd degree AV block Premature Ventricular Complex (PVC) Atrial Fibrillation Ventricular Tachycardia Ventricular Fibrillation Arrhythmias
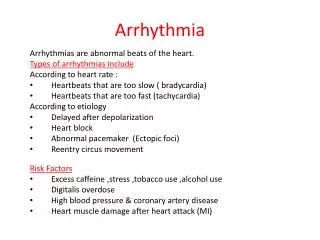
Pathological Conditions That Lead to Arrhythmias • Ischemia • Intracellular Ca2+ overload • Stress: adrenergic stimulation • Genetic defects- especially in ion channels • Anatomic defects • Drug effects
Bradycardia: Rate less than 60 • Disorders of impulse formation • Sinus bradycardia • Sinus node dysfunction (sick sinus syndrome • Junctional and ventricular escape rhythms • Disorders of impulse conduction (heart block) • 1,2,3 degree AV block
Sinus Bradycardia • Rate less than 60 • Normal P waves, PR interval • Causes: • Overmedication • Inferior wall MI • Increased intracranial pressure • Hypothyroidism • Carotid Sinus hypersensitivity • Normal Variant • Treatment: Atropine, external or tranvenous pacing if symptomatic, • EP of no value diagnosis is derived from Clinical Hx, clinical judgement, and monitoring and correlation with symptoms
1st Degree A-V Block • Not really “block” • Just P-R interval longer than normal (> 0.2 sec) • Treatment: none
2nd Degree AV BlockMobitz type 1 Some action potentials fail to get through the A-V node Normal Sinus Rhythm 2nd degree A-V block Treatment: none or ventricular pacing
2nd Degree AV Block Type I • Progressive PR interval lengthening • Dropped QRS • AV nodal delay
2nd Degree AV Block Type 2 • Constant PR interval • Dropped QRS • Infra-nodal delay- Treatment pacemaker
3rd Degree A-V Block No action potentials from the SA node/atria get through the A-V node Normal Sinus Rhythm 3rd degree A-V block Treatment: ventricular pacing
Junctional Rhythm • Originate from the area in and around the AV junction. • Inherent rate is 40-60 • Enhanced automaticity may causes more rapid rates. • Electrical impulses are conducted backward (retrograde) to depolarize the atria and forward (antegrade) to the ventricles. Makes the p-wave inverted in lead II.
Where are those P waves? • Impulse from AV junction depolarizes atria before ventricles - p waves will be in front of QRS • Impulse from AV junction depolarizes ventricles before atria - p waves will be after QRS • Impulse from AV depolarizes atria and ventricles simultaneously - p wave will be hidden in the QRS
Tachycardia: Rate Greater Than 100Causes • Increased automaticity: • atrial, junctional and ventricular premature complexes • Accelerated junctional rhythm • Accelerated idioventricular rhythm • Ectopic atrial rhythms • Some forms of VT • Triggered activity • Some forms of VT, long QT • Digoxin toxicity (Late after depolarizations) • Reentry • AV nodal reentrant tachycardia • AV reentrant tachycardia (WPW) • Atrial fibrillation • Atrial flutter • Most forms of VT
0 Action potential -50 200 msec Delayed Afterdepolarization (DAD) • Occurs only after a “triggering” action potential • Intracellular Ca2+ overload • ischemia • digitalis intoxication • adrenergic stress • Na/Ca exchange generating depolarizing current
0 Action potential Conduction times (1 mm/msec): 20 msec -50 A-C 10 msec A-B 10 msec C-B 10 msec 200 msec Normal Action Potential Conduction Purkinje fibers A 10 mm 10 mm 10 mm B C Ventricular Muscle
Re-entry Circuits as Ectopic Foci and Arrhythmia Generators • Atrio-Ventricular Nodal Re-entry • supraventricular tachycardia • Ventricular Re-entry • ventricular tachycardia • Atrial Re-entry • atrial tachycardia • atrial fibrillation • atrial flutter • Atrio-Ventricular Re-entry • Wolf Parkinson White • supraventricular tachycardia
Differential Diagnosis of Tachyarrhythmias Narrow complex: Regular-sinus tachycardia, ectopic atrial tachycardia, atrial flutter, junctional tachycardia, AVNRT, AVRT Irregular- Atrial fibrillation, multifocal atrial tachycardia, atrial flutter with variable conduction Wide complex Regular- Ventricular tachycardia, supraventricular tachycardia with aberrancy Irregular-Atrial fibrillation with aberrancy
Sinus Tachycardia • Sinus node is the pacemaker, firing regularly at a rate of greater than 100 times per minute. Each impulse is conducted normally through to the ventricles • Almost always occur as a response to some physiological stimulus (fever, exercise, volume depletion, thyrotoxicosis, hypotension • If symptomatic use AV nodal blocking agents (CCB,BB, Dig)
Atrial Flutter • Reentrant circuit around tricuspid valve • Flutter waves at 250-400 (avg 300/min) • AV conduction ratio 4:1, 3:1 ect • “Saw-toothed” waves • Treatment with ablation works around 99% of the time
Atrial Fibrillation • Irregular irregularity • R-R interval variablity • Rate greater than 400-600 • Two types-bad atrial tissue secondary to HTN, ischemia or bad pulmonary vein tissue young patients
Causes of Atrial Fibrillation • Pulmonary disease • Ischemia • Rheumatic heart disease • Anemia, atrial myxoma • Thyroid • Electrolytes • Sepsis
Atrial Fibrillation Treatment • Try to restore normal rhythm (cardioversion) only within 48 hrs • vagatonic maneuvers (carotid massage, Valsalva maneuver, gagging) • adenosine • If persistent rhythm: • control ventricular rate (calcium channel blocker, beta blocker) • anticoagulant therapy (coumadin)
Multifocal Atrial Tachycardia • Multiple P wave morphology • Multiple PR intervals • Irregular irregularity • Associated with COPD, hypoxia, and theophylline toxicity • Treat underlying cause, or AV node ablation with pacemaker
AV Nodal Reentrant Tachycardia • Results from a small micro-reentrant circuit within the AV node itself • Is usually initiated by a premature atrial beat • ECG tachycardia with no p waves or p waves after the QRS complex • Treatment is AV nodal-blocking drugs (CCB,BB,Dig)
Atrioventricular Reentrant Tachycardia • Involves a large reentrant loop with one limb of the circuit including the AV node and the other being an abnormal connection between the atria and ventricles (WPW) • Usually initiated by PVC • Two types- • Orthodromic (narrow complex QRS) 90%, Antidromic (wide complex QRS) 10% • IF AV nodal blocking agents are given with a-fib and avrt could cause V-fib
Ventricular Tachycardia • Usually associated with symptoms • Rate: 140-220 (200±50); at least 3 ectopic QRS in row • QRS: normally wide and bizarre • Usually associated with MI or other organic HD; unusual in normals • Often serious requiring quick treatment if sustained • Mechanism? Reentry or rapid firing ectopic?? • Treatment: cardioversion, lidocaine
Ventricular Fibrillation • Multiple foci in the ventricles become irritable and generate uncoordinated, chaotic impulses that cause the heart to fibrillate rather than contract. • Treatment: cardioversion
Asystole • The heart has lost its electrical activity. There is no electrical pacemaker to initiate electrical flow. • Treatment: ACLS protocol, transcutaneous pacing, epinephrine 1mg IVP q3 to 5, atropine 1mg q 3 to 5
Premature Atrial Contraction • Early beat that originates in the atria as an ectopic pacemaker • Etiology • Usually caused by enhanced automaticity in atrial tissue • May be a single or multiple ectopic sites • Shape of the p-wave depends on the location of the ectopic beat
Premature Atrial Contraction • P-wave configuration • Usually different from the underlying p-wave • QRS configuration • Usually similar to the underlying rhythm • If very early, the bundle branches may not have repolarized sufficiently for normal conduction. (usually conducted left and blocked right)
Non-compensatory pause * measurement between the R-wave preceding the PAC to the R-wave following the PAC is less than two R-R cycles of the underlying rhythm
Compensatory Pause * measurement between the R-wave preceding the PAC to the R-wave following the PAC equals two R-R cycles of the underlying rhythm
Antiarrhythmic Drugs • Class I: Local anesthetic action, reducing Na channel current • Lidocaine, Quinidine • Class II: b-Adrenergic antagonists • Propranalol • Class III: action potential prolongation • Amiodarone • Class IV - Ca channel antagonists • Verapamil
Quiz • Name the Rhythm # 1:
Answer: • Atrial Flutter