Download
1 / 25
250 likes | 269 Views
Secondary Syphilis (Dr. Bhushan Kumar). 35 year married male. Multiple asymptomatic, raised lesions about 2 cm in diameter on almost the whole body of 4 weeks duration. Ulcers over the prepuce and glans – 10 days.

E N D
Secondary Syphilis (Dr. Bhushan Kumar) • 35 year married male. • Multiple asymptomatic, raised lesions about 2 cm in diameter on almost the whole body of 4 weeks duration. • Ulcers over the prepuce and glans – 10 days. • Erythematous papular lesions appeared and spread rather quickly all over the body in about a week. Mild hyperpigmentation and scaling developed subsequently. Papular lesions on the prepuce and glans ulcerated subsequently. • Smoker. Sensitive to sulfa. • No history of extramarital contact.
Past history • Has genital ulceration about a year back which healed on its own in a few days. • Oral ulceration off and on. • No neurological, eye complaints, joint pains or systemic complaints. • Family history • history of genital ulceration in the wife twice in the past which healed of it own in a few days without any treatment.
GPE • Generalized lymphadenopathy – cervical , axillary, inguinal, epitrochlear • Multiple, discrete, rubbery, about 2 cm in size non tender mobile nodes.
Mucocutaneous examination Sites: Scalp, Face, Trunk, Extremities, and genitalia Morphology: • Multiple, well defined, discrete, oval to round, erythematous to copper coloured 1 cm to 2 cm infiltrated papuloplaque lesions covered with whitish fine scales over the face, trunk and extremities • Few lesions had a peripheral collarete of scales
Glans : Single well defined erythematous well defined round non tender non scaly .5 cm size papule • Prepuce : Two sharply marginated ulcers with indurated margins, non tender with necrotic slough at the base
Scalp: Few areas of non scarring alopecia • Oral mucosa : Normal • Nails: Normal • Palms and soles : Callosities present • Conjuncitva : Normal
PROVISIONAL DIAGNOSIS • Secondary syphilis
Investigations • Hematological and biochemical – NAD • DGI • Histopathology – secondary syphilis.
Investigations Patient serology • VDRL– Reactive (1:64) • TPHA– Reactive (>1:80) • HIV serology– Non-reactive • Skin biopsy– secondary syphilis Partner serology • VDRL – Reactive (1:16) • TPHA- Reactive (1:80) • HIV : Non reactive
Final diagnosis Secondary syphilis
Treatment • Counselling of patient • Single dose of Benzathine penicillin G 2.4 million units IM stat AST (1.2 MU in each buttock deep IM ) ↓ More than 90% of the lesions subsided within ten days • Lymph nodes also regressed in this period • VDRL on 10/3/2010 - 1:2 Treatment of partner • Single Dose of Benzathine Pencillin 2.4 million units IM stat AST (1.2 MU in each buttock deep IM )
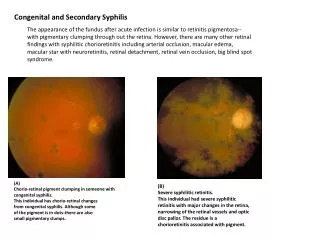
Discussion • Caused by spirochaete Treponema pallidum • Syphilis the “great imitator,” poses diagnostic dilemmas when it produces unusual skin lesions • It is of great chronicity, systemic from outset, capable of involving every sturcture of the body in its course, distinguished by florid manifestations on one hand and years of completely asymptomatic latency on other.
Mucous Membrane Lesions Oral features of secondary syphilis • Mucous patches • Maculopapular lesions • Nodular lesions may rarely arise.
Condylomata lata • Flesh-colored moist, oozing papules that become flattened and macerated .
Hair Abnormalities • Patchy moth eaten alpecia • Diffuse alopecia Moth-eaten alopecia
Differential Diagnosis of Secondary syphilis • Pityriasis rosea • Condyloma acuminata • Drug eruption • Viral Eruption • Psoriasis • Reiter syndrome
Management • Primary & Secondary Syphilis Recommended Regimen for Adults • Benzathine penicillin G 2.4 million units IM in a single dose Recommended Regimen for Children • Benzathine penicillin G 50,000 units/kg IM, up to the adult dose of 2.4 million units in a single dose
Management… Penicillin Allergy– Limited data to support the use of alternatives • Doxycycline- 100 mg BD for 14 days • Tetracycline -500 mg QID for 14 days • Ceftriaxone-1 g daily IM or IV for 8–10 days • Azithromycin- 2 g single oral dose • Pregnant patients who are allergic to penicillin should be desensitized & treated with penicillin
Follow-Up • Patients should be reexamined clinically & serologically at 6 months & 12 months • Patients who have signs or symptoms that persist or recur or who have a sustained fourfold increase in non-treponemal test titer probably failed treatment or were reinfected • These patients should be retreated & reevaluated for HIV infection
Management of Sex Partners • Persons exposed <90 days preceding the diagnosis even if seronegative should be treated presumptively • Persons >90 days before the diagnosis—Treated presumptively if serologic test results are not available & the opportunity for follow-up is uncertain