Download
1 / 40
400 likes | 420 Views
Learn about mental disorders caused by physical diseases, coping strategies, and the relationship between brain disorders and psychiatric symptoms in epilepsy. Explore how various general diseases can manifest as psychiatric symptoms.

E N D
Module Eight PSYCHIATRIC SYMPTOMS AND PHYSICAL DISEASES • Lesson 1: treatment of physical diseases and adapting to them • Lesson 2: Mental Disorders caused by a physical disease • Lesson 3: Epilepsy
Lesson 1 TREATMENT OF PHYSICAL DISEASES AND ADAPTING TO THEM
Step 1: Introduction Some mental disorders are a result of physical disease or damage which is either generalized or concerns only the brain. The psychiatric consequences of physical diseases can be separated in two categories: • Problems that derive from the treatment of physical disease or damage. • Mental disorders that derive directly from the physical disease or damage.
Step 2: Slide projection Slide 8.1.1: Patient’s behaviour This may comport: • visit to the doctor, • take medication, • stay in bed, • absence from work, • take advice from relatives and friends, • give up some activities.
Step 3 (continued) Slide 8.1.2: Coping and adaptation The psychological procedures that derive from short stressful events (which may include an illness) are known with the term coping, which practically means the way of getting along.
Lesson2 MENTAL DISORDERS CAUSED BY A PHYSICAL DISEASE
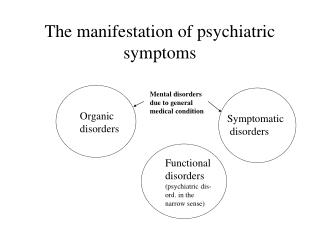
Step 1: Introduction • Many physical disorders can cause psychiatric symptoms similar to those characterizing mental disorders. • There are exterior natural factors, like medication (therapeutic or illegal) and other chemical substances that can too cause psychiatric symptoms. • The physical diseases related to the manifestation of psychiatric symptoms can be separated in brain disorders and general or systematic Disorders even though in reality these two categories overlap.
Step 2: Slide projection Slide 8.2.1: Brain disorders with psychiatric symptoms • Acute confusional state Delirium • Chronic brain syndromes Dementias • Focal disorders Tumors, Vascular events • Brain disorders that cause symptoms of other psychiatric disorders. Epilepsy
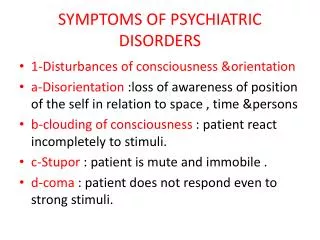
Step 3: Theory presentation Acute confusional state (delirium) • Common in pathological and surgical units (5 – 15%) and in Intensive treatment units (20-30%). • The person is disorientated, cannot remember some things and is uneasy and shows hyperactivity, irritability, fear or aggression, even delusions or hallucinations and ideas of persecution. • There are many causal factors: Medication, General infections, Brain infections, Kidney failure, Hepatic failure, Brain tumors, Cerebrovascular episodes, Cerebral injuryEpilepsy.
Step 3 (continued) Chronic brain syndromes • It is about dementias, which are already described. Dementias do not appear only to elders, some of them can also appear to people of other ages. • The causes of dementias include many factors that cause deliriums.
Step 3 (continued) Focal Disorders • The disorder or injury is found in a section of the brain and the symptoms depend on the principal functions of this section. • The disorders related to a particular brain section are more common after brain injury, cerebrovascular injuries, or tumors.
Step 3 (continued) Brain disorders that cause symptoms of other mental disorders. • The symptoms of delirium or dementia focus on orientation and memory. Other disorders, though, cause psychiatric symptoms similar to Schizophrenia’s, Mania’s or Depression’s. • The most common of these disorders is Epilepsy. Apart from confusional symptoms that appear during generalized seizures, it can cause delusions. Epilepsy of temporal lobecan lead to escape behaviour, like in Conversion Disorders.
Step 4: Slide projection Slide 8.2.2: General diseases with psychiatric symptoms • Diseases from vitamins deficiency (pellagra, deficiency B1, deficiency B12) • Endocrine disorders(Cushing's syndrome, hyperthyroidismand hypothyroïdism, Addison disease, pheochromocytoma , hyper and hypoparathyroidism, hypopituitarism) • Drugs and toxic substances • Infections (Syphilis, Aids, Malta fever, glandular fever, HIV infection) • Metabolism disorders ( hepatic insufficiency, electrolyte disorders, uraemia) • Acute intermittent porphyria • Multiple sclerosis • Lupus erythematosus
Step 5: Slide projection and Discussion Slide 8.2.3: Psychiatric symptoms of physical disorders Schizophrenic Symptoms: Delirium, Dementias, Brain tumors, Cerebrovascular episodes, Brain lesions, Epilepsy, Cushing syndrome, Hyperthyroidism, Hypothyroïdism, hypoparathyroidism, Medication and toxic substances,Syphilis, Aids, multiple sclerosis, Hepatic insufficiency, Hypoglycaemia, electrolyte disorders, uraemia, acute intermittent porphyria, lupus erythematosus
Step 5 (continued) Depression: Brain tumors, Epilepsy, Deficiency B12, Cushing’s syndrome, Hypothiroïdisme, Addison disease, Hyper parathiroïdisme, Hypopituitarism, Medicationand toxic substances, Syphilis, Aids, Malta fever, monocytic angina, hepatitis, multiple sclerosis, Electrolyte disorders, Uraemia, Acute intermittent porphyria
Step 5 (continued) Manic symptoms: Brain tumors, B1 deficiency, Cushing syndrome, Medication and other substances, Syphilis, Aids, Multiple sclerosis, Acute intermittent porphyria
Step 5 (Continued) Anxiety Symptoms: Cushing syndrome, Hyperthyroidism, Pheochromocytoma, Aids
Lesson3 EPILEPSY
Step 1: Slide projection Slide 8.3.1: What is Epilepsy? Epilepsy is a chronic or recurrent disorder, which is related to the state of consciousness and depends on the electrical excitations activity of the brain.
Step 1 (continued) From these that have Epilepsy: • 70-80% have no episodes after the therapy • 20% is difficult to treat • 80% take medication
Step 2: Discussion 1 in 3 persons that suffer from Epilepsy appear some psychiatric problems. This correlation is even higher for temporal lobe Epilepsy. • Why is the occurrence of psychiatric symptoms in persons with Epilepsy so high? • What is the connection between mental disorders and Epilepsy?
Step 2 (continued) • People who suffer from epilepsy face difficulties to join into society because of their state. • The medication they are on aggravate these difficulties. • The appearance of psychotic episodes people with temporal lobe epilepsy is common and it is considered in these cases that both are caused by the same physical problem. • Epileptics appear more often high rate of mental retardation and personality disorders, which are again attributed to the same physical problem and to medication.
Step 3: Slide projection Slide 8.3.2: Cause of epilepsy Unknown : 70% (some cases might be hereditary) Rest : 30% Brain lesion Metabolic causes
Step 4: Theory presentation and slide projection There are different types of epileptic seizures. A person that suffers from Epilepsy might show more than one type of epileptic seizures but usually there is a standard and particular type for this person. The type of seizures depends on the brain section that is injured. According to International classification of Seizures, the seizures can be classified as Partial and Generalized.
Step 4 (continued) Partial seizures • Simple • Complex Generalized seizures • With tonic clonic spasms (known in the past as grand mal) • Muscle contractions • Drop attacks • Reductions (known aspetit mal) • Muscle spasms Secondary Generalized seizures
Step 5: Discussion In most epileptic persons the seizures are not predictable but there might be dissolute factors. What are the most frequent dissolute factors? • Psychological: Stress, fatigue, anxiety, boredom, agitation, sadness. • Physical: bad health, hormonal changes, constipation, nutrition changes. • Environmental: flashing lights, television, images with geometric shapes, sounds, intense heat or cold.
Step 6: Slide projection Slide 8.3.4: Seizures’ description • Is there any warning sign before the seizure? • What has happened before the seizure? • What happens when the seizure is finished? • How exactly is the seizure?
Step 7: Theory presentation and Slide projection Slide 8.3.5: Tests Εξετάσεις • Physical and psychiatric diagnosis • EEG (Electroencephalograph ) • Cranial Imaging (CAT, MRI) • Psychological research • Detailed History • Seizures observation
Step 7 (continued) EEG - (electroencephalograph ) • Records images of electric clearing evacuation from brain’s nervous cells. • It is used as means for neurologic disorders’ diagnosis. • A common EEG usually lasts for about 25 minutes. • The person is asked to open and close its eyes and take deep breath or look in flashing lights. • It can help to differentiation from other disorders and to the classification of the Epileptic type. • A normal EEG can never totally exclude Epilepsy.
Step 7 (continued) Cranial Imaging Techniques • Computed Tomography (CT) – fit for brain structure anomalies. • Magnetic Tomography (MRI) – eases the differential diagnosis
Step 7 (continued) Psychological research It is done with neuropsychological tests and psychometric Tests. The EEG, and simultaneous psychometric tests, can contribute to identification of the epileptic centre and of its effects to cognitive functions.
Step 8: Slide projection Slide 8.3.6: Treating an epileptic seizure You have to : • Loosen his/ her clothes. • Lift up his/ her head – even by putting his/ her hands under it if there is no other way. • Turn the person to its side after the seizure – this helps breathing. • Move any furniture or objects that may injure the person.
Step 8 (continued) You must not: • Move the person during the seizure, except if there is danger. • Put any object between his/ her teeth. • Restrain his/ her movements. • Abandon the person until he / she is perfectly well. • Give something to drink or eat until is perfectly well.
Step 8 (continued) Slide 8.3.7: Antiepileptic medication • Valproic Acid(Depakine) First rate:primary-reductions, muscle spams, tonic spasms, Second rate: Focal, All • Carbamazepine(Tegretol) First rate:Focal Second rate: tonic spasms • Phenitoin sodium (Epanutin) First rate: Focal, origin tonic spasms
Step 8 (continued) • Phenobarbital (Gardenal) Secondary rate: Focal, Generalized tonic spasms • Primidone (Mysoline) Secondary rate: Focal, Tonic spasms • Clonazepam (Rivotril) Secondary rate: Reductions, Muscle spasms, All • Gabapentin (Neurontin) • Lamotrigine(Lamictal) Secondary rate: Resistant, Focal, Generalized
Step 8 (continued) Side effects of antiepileptic medication. The eventual severe side effects are depression, ataxia, and hematological disorders. The milder social side effects of these medication are hypertrichosis, obesity, oedema of the gums and hardness of facial characteristics.
Step 8 (continued) • The efficiency of the medication depends on the levels of the medication in the blood, not by the way it is taken. It is possible to measure the medication level in the blood. • Many people need to take antiepileptic medication for all their life, the doctor can decide to stop it if the person is free of seizures for two years. The general rule for every change or stop of the medication is “ the slightest change possible within the longest possible time period”.