Download
1 / 33
330 likes | 405 Views
Bronchiectasis. Northland. 2013 - 10 known paediatric patients with bronchiectasis in Whangarei and 4 in greater Northland. Now 27 confirmed non cystic fibrosis bronchiectatic patients in Northland. Early and effective management reduces short- and long-term morbidity. Definition.

E N D
Northland • 2013 - 10 known paediatric patients with bronchiectasis in Whangarei and 4 in greater Northland. • Now 27 confirmed non cystic fibrosis bronchiectatic patients in Northland
Early and effective management reduces short- and long-term morbidity
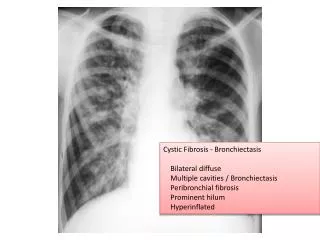
Definition • Irreversible bronchial dilatation • Radiological or pathological diagnosis • HRCT scan current gold standard
Chronic Suppurative Lung Disease • Symptoms of chronic endobronchial suppuration +/- radiological evidence of bronchiectasis
Chronic infective bronchitisProtracted bacterial bronchitis • Prolonged wet cough • Resolves completely after treatment • If untreated may progress to bronchiectasis
Bx, CSLD, Protracted bacterial bronchitis • Symptoms and signs overlap and lack specificity • Absolute reliance on radiology-based definition unsatisfactory • When to do imaging • Age related changes in bronchoarterial ratio uncertainty • 2 HRCT scans to fulfil irreversible defn • Influence of acute illness
Definitions • ?chronic suppurative lung disease best overarching term
Pathogenesis • Obstruction • Chronic inflammation, progressive wall damage, dilatation • Abnormal cartilage formation (congenital causes) • Common thread: difficulty clearing secretions + recurrent infections • Resulting airway injury and remodelling
Pathogenesis 2 • Infections and an ineffective host immune response involving uncontrolled recruitment and activation of inflammatory cells within lower airways • Release of mediators, eg proteases and free radicals • Causing bronchial-wall injury and dilatation
Causes (paeds) • Congenital • CF • Immune deficiency • Primary ciliary dyskinesia • Aspiration, recurrent small volume • Post-infection • (Systemic inflammatory diseases)
Investigations • FBC • Immunoglobins • Sweat test • Sputum • PCD – exhaled fractional nasal nitric oxide and/or nasal ciliary brushings • Spirometry and lung volumes (>6yo)
Invx additional • CF gene mutations • Bronchoscopy – FB/ airway abnormality • Ba swallow/ video fluoroscopy • Further immune tests • IgE, neut fnc test, lymphocyte subsets, ab resp to vaccinations • HIV • Echo (esp adults, ?pulm hypertension)
Assessment of severity 1 • Clinical • Cough • Sputum • Exacerbation rate • Well-being
Assessment Severity 2Lung function • Spirometry • Classically obstructive • Repeated at each review • Relatively insensitive in mild disease, and in children • Spirometric volumes can stabilize and improve in children • 6 minute walk • Assessment functional impairment
Microbiology • Common pathogens children: • H influenzae • S pneumoniae • M catarrhalis
Management Early and effective mgmt reduces short- and long-term morbidity
Management 1 • Airway clearance Chest physiotherapy • Nutrition • Fitness and activity • Avoidance of environmental pollutants • TOBACCO • Assessment for co-morbidities • Annual ‘flu immunisation
Management 2 • Intensive antibiotic treatments • Reduce microbial load • Oral Abx and ambulatory care initially • Hospital and IV Abx + intensified physio • more severe/ unresponsive oral
Burden of diseaseIncidence – non-CF Bx/CSLD • NZ <15yo 3.7/100 000 per year (2x CF incidence) • Central Australian Indigenous children 1470/1000 000/year • US 18-34 yo 4.2/100 000
Northland • 27 children 0-16 • Almost all post-infection • x1 with unsafe swallow • x1 with IgA deficiency • 2 other children with PCD but not Bx
Paediatric Bronchiectasis Clinic • Quarterly multidisciplinary clinic • Currently only at Whangarei • Physio, nurse, doctor • Team meeting at the conclusion of each clinic to discuss patient’s plans and monitoring and discussion of issues. • Same physiotherapist in clinic as on ward • aids with continuity of care • outreach nurse also follows patient both in the community and on admissions.
Aims of Multidisciplinary clinic: • To provide standardised care to children with bronchiectasis • To provide ongoing monitoring in accordance with guidelines for bronchiectasis • To prevent/reduce hospital admissions • To provide a continuum of physiotherapy techniques in the management of bronchiectasis through their childhood
Aims of Multidisciplinary clinic • To develop a proactive application to deliver health care for these children and their families to reduce disease progression • To provide education and promotion of healthy lifestyles for families with the aim of reducing disease progression • To provide a central point of contact for patients and family with bronchiectasis and thus patient centred care • To provide holistic care • To reduce inequalities of health care access
Presentation • Chronic or recurrent wet cough • Children do not usually expectorate • Cough often temporarily resolves after treatment
Primary care input 1 • Index of suspicion • Two or more episodes of chronic (>4 wks) wet cough/year that respond to Abx • CXR abnormalities persisting at least 6 wks after appropriate therapy • Specialist referral
Primary care input 2 • Management of exacerbations • Appropriate antibiotic for patient • Appropriate length of course • Low threshold for referral for admission if not improving • Routine immunisations, plus annual ‘flu • Smoking cessation advice and support