Download
1 / 55
550 likes | 713 Views
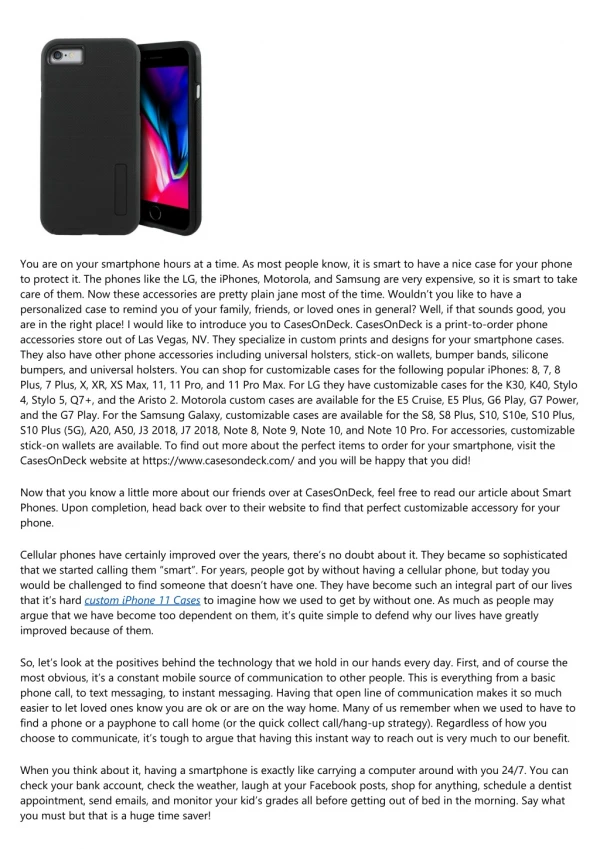
Roman Perez-Soler, MD Montefiore Medical Center Albert Einstein College of Medicine. Personalized Therapeutic Approaches for NSCLC Case Discussions. Disclosure Slide. Case 1: Adenocarcinoma, wt EGFR, Cavitated Primary Tumor. 59-year-old female, smoker 20 pack x year

E N D
Roman Perez-Soler, MD Montefiore Medical Center Albert Einstein College of Medicine Personalized Therapeutic Approaches for NSCLCCase Discussions
Case 1: Adenocarcinoma, wt EGFR, Cavitated Primary Tumor • 59-year-old female, smoker 20 pack x year • Chest pain, weight loss, PS 1, no hemoptysis • Bronchoscopy: Adenocarcinoma, wt EGFR • Stage IV: T2 N2 (R mediastinum) M1 (bone, adrenals) • No brain metastases
Possible Options • Paclitaxel/carboplatin/bevacizumab (Phase III, E4599) • Pemetrexed/cisplatin (Phase III, Scagliotti et al) • Vinorelbine/cisplatin/cetuximab (Phase III, FLEX) • Docetaxel/cisplatin (Phase III, TAX 326) • Pemetrexed/carboplatin/bevacizumab (Phase II, Patel et al)
Case 1: Follow-Up • Patient was treated with carboplatin, paclitaxel and bevacizumab and achieved a partial response after 2 cycles
Case 1: Follow-Up • Patient completed 4 cycles of therapy and was put on bevacizumab maintenance • Patient progressed after 4 cycles of bevacizumab maintenance, started erlotinib, had stable disease for 5 months, progressed and was treated with pemetrexed
Discussion Points • What is the best chemotherapy in combination with bevacizumab in NSCLC? • What are the current contraindications for the use of bevacizumab in NSCLC? • Is the type of non-squamous histology important for the use of bevacizumab? • Why not treat this patient with pemetrexed + cisplatin given the 2-month median survival superiority over gemcitabine + cisplatin in Scagliotti’s study? • Would switch maintenance therapy with pemetrexed or erlotinib be a reasonable option for this patient? • Are there any biomarkers to predict bevacizumab antitumor efficacy? • Should this tumor be tested for the ALK translocation nowadays?
Comments (1) • Carboplatin/paclitaxel is the only chemotherapy regimen with which bevacizumab has shown to have an impact on survival. • Main current contraindications for the use of bevacizumab are squamous histology, hemoptysis and history of severe cardiovascular disease. • Tumor cavitation, brain metastases and use of anticoagulation are not contraindications. • Best survival results in E4599 were observed in patients with adenocarcinoma (14 vs 10 months).
Comments (2) • The use of cisplatin + pemetrexed as front-line therapy has emerged more recently as an excellent option but precludes the use of bevacizumab for the treatment of this patient as bevacizumab is only approved and has only shown clinical benefit as front-line therapy. • Switch maintenance is a form of early second-line therapy and appears to benefit more patients with stable disease with front-line therapy than patients with a response to front-line therapy. • There are no biomarkers predictive of bevacizumab efficacy in NSCLC. In other tumors, VEGF levels have been found to be predictive of efficacy. • The ALK translocation should be analyzed in oligosmokers who have wt EGFR tumors.
Case 2: Adenocarcinoma, Brain Mets, wt EGFR • 61-year-old female, 80 pack x year tobacco use, quit 1 year ago, well-controlled hypertension, no hemoptysis • Dizziness, ataxia • MRI brain: Large cerebellar tumor, numerous bilateral brain metastases • PET/CT: RUL mass, bilateral pulmonary nodules, liver metastases • Resection of cerebellar tumor • Histology: Adenocarcinoma, wt EGFR, ALK translocation not tested
Case 2: Adenocarcinoma, Brain Metastases, EGFR wt — Follow-Up • Whole brain XRT: Asymptomatic off dexamethasone • Started on pemetrexed/carboplatin/bevacizumab • Good tolerance to treatment, except significant nausea • Remarkable response after 4 cycles
Discussion Points • Is pemetrexed + carboplatin + bevacizumab a reasonable option for this patient?
Pemetrexed/Carboplatin/Bevacizumab Pemetrexed* Carboplatin Bevacizumab 15 mg/kg x 6 cycles PD/toxicity Off study CR/PR/SD Pemetrexed* Bevacizumab 15 mg/kg until PD or unacceptable toxicity Primary endpoint: PFS *Vitamin B12, folate and dexamethasone given Patel et al. ASCO 2008
Comment • The combination of pemetrexed + cisplatin is superior to gemcitabine + cisplatin in patients with adenocarcinoma histology (Scagliotti study). • The best survival results in E4599 were observed in patients with adenocarcinoma, with little impact observed in other non-squamous histologies. • Although there is only Phase II data supporting the use of bevacizumab with pemetrexed combinations, these two observations have led to the widespread use of pemetrexed + bevacizumab combinations for the treatment of patients with adenocarcinoma.
Discussion Points • Is pemetrexed + carboplatin + bevacizumab a reasonable option for this patient? • Is continuation maintenance pemetrexed a reasonable option for this patient?
Comments • Continuation maintenance with pemetrexed has been recently reported to prolong PFS in patients with non-small cell lung cancer (PARAMOUNT study). • In contrast with switch maintenance therapy, continuation maintenance is a form of therapy intensification and as such appears to benefit mostly those patients who achieve a response with front-line therapy. • Therefore, this patient would be a good candidate for continuation pemetrexed maintenance therapy.
Paramount: Study Design Study Treatment Period Progression Induction Therapy (4 cycles) 21 to 42 Days Maintenance Therapy (Until PD) 500 mg/m2 Pemetrexed + BSC, d1, q21d • Patients enrolled if: • Nonsquamous NSCLC • No prior systemic treatment for lung cancer • ECOG PS 0/1 CR, PR, SD 2:1 Randomization Placebo + BSC, d1, q21d • Stratified for: • PS (0 vs 1) • Disease stage (IIIB vs IV) prior to induction • Response to induction (CR/PR vs SD) 500 mg/m2 Pemetrexed +75 mg/m2 Cisplatin, d1, q21d PD • Randomized, placebo-controlled, double-blind, Phase III study • Folic acid and vitamin B12 administered to improve pemetrexed tolerability PD: progressive disease, BSC: best supportive care, CR: complete response, PR: partial response, SD: stable disease, NSCLC: non-small cell lung cancer, ECOG: Eastern Cooperative Oncology Group, PS: performance status
Investigator-Assessed Progression-Free Survival (Induction Phase) *UnadjustedBSC = best supportive care
Case 2: Adenocarcinoma, Brain Metastases, wt EGFR — Follow-Up • Continued on pemetrexed/bevacizumab maintenance • Developed thrombocytopenia that required pemetrexed dose reduction • PD after 6 cycles of pemetrexed/bevacizumab maintenance, started on erlotinib, no response • ALK translocation not tested
Case 3: Second-Line TreatmentSquamous Cell Carcinoma • 68-year-old white male, smoker since age 21, current smoker of 1 pack/day • Presents with 2.5 cm-spiculated peripheral mass in RUL, no clear hilar adenopathy • PET/CT: Bilateral adrenal metastases • CT brain negative • Bronchoscopy: Squamous cell carcinoma • PS 2: Cough, SOB on exertion, weight loss • Started on carboplatin + paclitaxel: PD in lung and adrenal glands after 2 cycles
Case 3: Squamous Cell Carcinoma — Options • Docetaxel • Erlotinib • Docetaxel + cetuximab
Case 3: Squamous Cell Carcinoma — Follow-Up • Started on erlotinib • Symptom improvement • No skin or GI toxicity • Stable disease at 8 weeks • Continues to smoke
Case 3: Squamous Cell Carcinoma — Options • Docetaxel • Increase erlotinib to 200 mg • Continue erlotinib at 150 mg • Supportive care
Discussion Points • Is vinorelbine + cisplatin + cetuximab a better option than carboplatin + paclitaxel in a patient with squamous carcinoma? • Is erlotinib inferior to docetaxel in this setting? • Is there a rationale for erlotinib dose adjustment? • Are there any new agents with a preferential activity against squamous carcinoma?
Comments • Cetuximab is the only targeted agent that has shown to add to chemotherapy in patients with squamous carcinoma (FLEX study). • EGFR expression by IHC staining has been recently shown to be a predictor of benefit with chemotherapy + cetuximab (IHC score >200). • Erlotinib has similar activity to docetaxel in non-selected patients in the second-line setting and is less toxic. • Current smokers must quit smoking before starting erlotinib or must have the erlotinib dose adjusted. • Several new agents have shown preliminarily a preferential activity against squamous carcinoma.
FLEX: OS — Caucasians (N = 946)Prespecified Analysis p-value: stratified log-rank test (2-sided) CV = cisplatin/vinorelbine Pirker. ASCO 2008 (abstr 3).
Survival in the High EGFR Expression Group (N = 345) Hazard ratio = 0.73 (95% CI 0.58-0.93); p = 0.011 Pirker R, Paz-Ares L. Proc IASLC 2011;Abstract 1557.
Erlotinib Is Effective in Both Squamous and Non-Squamous Tumours • Adenocarcinoma: HR = 0.7; p = 0.008* • Squamous: HR = 0.67; p = 0.0007* *Log-rank test Shepherd FA et al. N Engl J Med 2005;353(2):123-32.
Comparison of Phase III Trials in Relapsed NSCLC: Efficacy* Erlotinib and chemotherapy have similar efficacy in the second-line setting * Results cannot be compared directly because of different patient populations 1 Shepherd F et al. N Engl J Med 2005;353:123–32; 2 OSI and Roche data on file; 3 Shepherd F et al. J Clin Oncol 2000;18:2095–103; 4 Fossella F et al. J Clin Oncol 2000;18:2354–62; 5 Hanna N et al. J Clin Oncol 2004;22:1589–97.
Phase III TITAN-SLS (BO18602): Erlotinib in Treatment of Advanced NSCLC — Second-Line Setting Tumour samples Erlotinib 150 mg/day PD Off study 4 cycles of first-line standard platinum-based doublet Chemotherapy naïve Stage IIIb/IV NSCLC PD Pemetrexed or docetaxel PD Off study Non-PD SATURN • Primary endpoint = OS • Secondary endpoints = PFS, RR, QoL (FACT-L), correlation of biomarkers with clinical outcome Ciuleanu T et al. Chicago Multidisciplinary Symposium in Thoracic Oncology, Dec 2010 (Abs. LBOA5)
Similar OS with Second-Line Erlotinib and Chemotherapy in EGFR wt NSCLC: TITAN • Erlotinib (n = 75), median OS = 6.6 months • Chemotherapy (n = 74), median OS = 4.4 months • Hazard ratio = 0.85 Ciuleanu T et al. Chicago Multidisciplinary Symposium in Thoracic Oncology, Dec 2010 (Abs. LBOA5)
PKs of Erlotinib in Smokers versus Non-Smokers (Healthy Volunteers) • Single dose of erlotinib 150 mg AUC0–∞ non-smoker (18,726 ng•h/mL) AUC0–∞ smoker (6,718 ng•h/mL)p < 0.0001Exposure in smokers versus non-smokers = 35.9% Cmax non-smoker (1,056 ng/mL) Cmax smoker (689 ng/mL)p = 0.310 Maximum exposure in smokers versus non-smokers = 65.2% • Likely explanation: Cigarette smoke induces CYP enzymes responsible for metabolism of erlotinib Hamilton et al. Proc Am Assoc Cancer Res 2005. Hamilton et al. Clin Cancer Res 2006.
Agents with Claimed Preferential Activity in Squamous Cell Carcinoma • Anti IGF-1R antibody: Figitumumab • Nab paclitaxel • Anti CTLA-4 antibody: Ipilimumab
Case 3: Squamous Cell Carcinoma — Follow-Up • Patient was convinced to quit smoking • Erlotinib dose was increased to 200 mg and rash Grade 1 was noted • Patient had SD for 6 months and then progressed
Case 4: Adenocarcinoma, EGFR Mutant • 76-year-old female, Chinese, never smoker • Presents with shortness of breath • PET/CT shows large R pleural effusion, RLL mass and R mediastinal adenopathy • PS 1, no hemoptysis, no brain metastases • Pleural fluid: Adenocarcinoma, EGFR mutation analysis pending • Stage IVa adenocarcinoma
Case 4: Adenocarcinoma, Never Smoker, EGFR Pending — Options • Paclitaxel/carboplatin/bevacizumab • Pemetrexed/cisplatin • Wait for EGFR mutation analysis • Erlotinib
Case 4: Adenocarcinoma, Never Smoker, EGFR Pending/Mutant • Started with paclitaxel/carboplatin/bevacizumab • Good tolerance to first cycle of treatment • EGFR mutation test reported before cycle #2: Exon 19 deletion • Patient continued on paclitaxel + carboplatin + bevacizumab: SD after 2 cycles, PD in lung lesion after 4 cycles
Case 4: Adenocarcinoma, EGFR Mutant • Started on erlotinib 150 mg • Symptom improvement at one week; skin rash Grade 2 at 2 weeks • Tumor response on PET/CT at 6 weeksContinues with minimal residual disease on erlotinib 150 mg at 36 months
Case 5: Adenocarcinoma, EGFR Mutant • 62-year-old male from Dominican Republic; 5 pack x year smoking history, quit 38 years ago • Presents with headache at another hospital • MRI shows multiple brain metastases • PET/CT shows spiculated LUL mass: FNA shows adenocarcinoma • Tumor sent for EGFR testing • Whole brain radiotherapy • Pemetrexed + cisplatin x 2: No response
Case 5: Adenocarcinoma, EGFR Mutant • Referred to our Institution • EGFR mutations analysis results received after starting first cycle of chemotherapy show exon 19 deletion • Started on erlotinib 150 mg • Develops Grade 2 rash and Grade 3 paronychia: Dose adjusted to 100 mg • Complete remission at 6 weeks • Last follow-up at 18 months shows no evidence of disease in brain and lungs • Continues with erlotinib 100 mg with Grade 1 rash
Discussion Points • Unless patients are highly symptomatic, physicians should wait for results of EGFR mutation analysis before starting therapy with chemotherapy • Both patients did not respond to front-line chemotherapy • Caucasian patients with EGFR-mutated tumors have a very low response to chemotherapy (15%, EURTAC study, ASCO 2011) • What are the options for tumors that develop resistance to erlotinib?
EURTAC Study Design EURTAC; NCT00446225 Erlotinib 150 mg/day PD • Chemonaїve • Stage IIIB/IV NSCLC • EGFR exon 19 deletion or exon 21 L858R mutation • ECOG PS 0–2 • (n = 174) Stratification • Mutation type • ECOG PS (0 vs 1 vs 2) R Platinum-based doublet chemotherapy q3w x 4 cycles* PD • Phase III, randomised, open-label, active-controlled • Primary endpoint • Progression-free survival (PFS) • Interim analysis planned at 88 events • Secondary endpoints • Objective response rate (ORR) • Overall survival (OS) • Location of progression • Safety • EGFR mutation analysis in serum • Quality of life (QoL) *Cisplatin 75 mg/m2 d1/docetaxel 75 mg/m2 d1; cisplatin 75 mg/m2 d1/gemcitabine 1,250 mg/m2 d1,8;carboplatin AUC6 d1/docetaxel 75 mg/m2 d1; carboplatin AUC5 d1/gemcitabine 1,000 mg/m2 d1,8. With permission from Rosell R et al. Proc ASCO 2011;Abstract 7503.