Download
1 / 65
650 likes | 661 Views
Learn about neurodegenerative disorders, like multiple sclerosis (MS), and Parkinson's disease, their symptoms, available treatments, and care strategies. Discover the impact on daily life and ways to support sufferers effectively.

E N D
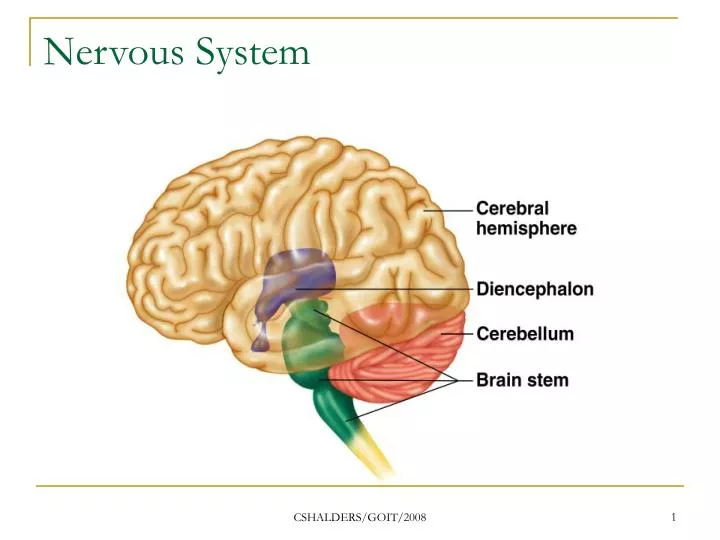
Nervous System CSHALDERS/GOIT/2008
Neurodegenerative Disorders • Can cause morbidity and mortality • Most of these disorders produce a progressive deterioration in neuronal function and tend to be irreversible CSHALDERS/GOIT/2008
Multiple Sclerosis • Etiology unknown • The disease affects the white matter of the spinal cord and the brain, where autoimmune activity causes lesions CSHALDERS/GOIT/2008
Multiple Sclerosis • Wide variation in clinical manifestations and prognosis • Progressive form – which continually worsens with no remission • Relapsing – remitting from- characterised by a serious of attacks followed by partial remission CSHALDERS/GOIT/2008
Multiple Sclerosis (MS) • Autoimmune disorder causing destruction of myelin sheaths in CNS • appears between ages 20 and 40 • females twice as often as males • Symptoms include muscular weakness, stiffness. Parathesias, pain and muscle spasm are observed. • Emotions, memory vision motor coordination also affected CSHALDERS/GOIT/2008
Multiple Sclerosis • Survival time from diagnosis can be well over 20 years so important to offer sufferers • Every aid to improve their quality of life • Because the disease is autoimmune best causative treatment involves use of immunosuppressive drugs CSHALDERS/GOIT/2008
Multiple Sclerosis • Two specific immunosuppressive drugs used in MS are glatiramer and interferon • Both these drugs can reduce the number of relapses • Are given by subcutaneous injection CSHALDERS/GOIT/2008
Multiple Sclerosis • Glatiramer • Modify the immune process • 20 mg s/c daily • Adverse effects • Injection site reactions, vasodilation, taccycardia, palpitations, chest pain • Prec: Should not be given IV or IM • Rotate injection sites CSHALDERS/GOIT/2008
Multiple Sclerosis • Interferon β 16 • Requires monitoring complete blood count and liver function at baseline at three months at six months • Adverse effects • Flu like symptoms, lethargy weakness and fatigue. CSHALDERS/GOIT/2008
Multiple Sclerosis Dantrolene • Works as a muscle relaxant, interferes with release of calcium ions from skeletal muscle • Prec – hepatic disease, pre, BF photosensitivity • AR – drowsiness, dizziness, malaise GI • Inter – OC, alcohol verapamil, tranquilizers • Pres – 25mg 50 mg • Dose – Adult 25mg daily ^ to 50 mg – 100mg 3-4 * daily CSHALDERS/GOIT/2008
Multiple Sclerosis • Baclofen • Used for spasms • Antispasticity agent that acts on the spinal end of the upper motor neuron • Adverse effects • Nausea, vomiting, dry mouth, constipation • Considerations: take with food do not stop abruptly CSHALDERS/GOIT/2008
Multiple Sclerosis • Amantadine • For fatigue • Thought to stimulate the release of dopamine in the brain • Adverse effects- palpitations, hypotension, peripheral oedema • Considerations: Watch for postural hypotension CSHALDERS/GOIT/2008
Multiple Sclerosis • Corticosteroids such as prednisolone or methylprednisolone can be effective in acute phases • Aggressive antibiotic therapy used for infections • Tricyclic antidepressants used for depression • Propantheline for urinary urgency CSHALDERS/GOIT/2008
Parkinsons Disease • Named after a Doctor who discovered the disease • Cause is unknown research has shown a reduction in the dopamine in the brain which prevents correct brain cell function • Characterized by tremors and progressive muscle rigidity CSHALDERS/GOIT/2008
Parkinsons • Seen to affect more men than women • Middle age or later • Genetic factors ?viruses and environmental toxins • The reduction in dopamine leaves an excess of acetylcholine that causes over excitation • Dopamine receptors degenerate, causing excessive muscarinic activity CSHALDERS/GOIT/2008
Parkinsons • The seesaw remains unbalanced, as the dopaminergic activity is never sufficient to keep the seesaw in balance • This is the essence of parkinsons disease pathophysiology CSHALDERS/GOIT/2008
Parkinsons • To treat is to rebalance the seesaw • Two methods • Decrease the muscarinic activity and or increasing the dopaminergic activity CSHALDERS/GOIT/2008
Parkinsons • Aim of most drugs is to increase the amount of dopamine produced and available to the cerebral tissues • Levodopa is the precursor to dopamine • Can cross the blood brain barrier where it is converted into dopamine • The enzyme that converts levodopa to dopamine is decarboxylase CSHALDERS/GOIT/2008
Parkinsons • By giving large doses of levodopa the dopamine produced triggers severe peripheral adverse effects • To combat this carbidopa and benserazide unable to cross the blood brain barrier • We add one of these compounds to levodopa the peripheral conversion of levodopa to dopamine is inhibited, allowing more levodopa to cross the blood brain barrier CSHALDERS/GOIT/2008
Parkinsons • Ergot derivatives medications are also used in parkinsons disease to stimulate central dopamine receptors • Helps reduce muscle rigidity, but is less effective than levodopa CSHALDERS/GOIT/2008
Parkinsons • Carbidopa/Levodopa (Sinemet) • Used for treatment of parkinsons disease • Contra:Maoi’s glaucoma, melanoma • Pre: Ph psychotic episodes, convulsion, peptic ulcers,antihypertensives, arrythmias,asthma, preg, severe cardiac, renal pulmonary. • AR: muscle twitching depression • Inter: MAOI’s, tricyclics, iron, phenytoin,intal CSHALDERS/GOIT/2008
Parkinsons • Side effects of levodopa include nausea, depression, agitation and confusion as well as involuntary movements of the head lips and tongue. • Some of these effects can be avoided by using slow release preparations, which maintain more constant blood levels CSHALDERS/GOIT/2008
Parkinsons • The effect of levodopa tends to decrease with time until no effect is produced at all • Therefore the drug is given more frequently • This is probably due to progressive degeneration of the dopaminergic neurones CSHALDERS/GOIT/2008
Parkinsons • Levodopa should be taken at the same time each day and always with food to ensure uniform blood concentrations of levodopa Long term levodopa therapy can cause • On –off phenomenon where marked symptoms develop, for a period of time before normality returns. CSHALDERS/GOIT/2008
Parkinsons • Benzhexol (Artane) • Anticholernergic agent, relaxing effect on smooth muscle • Prec: cardiac dys, renal dys, hepatic dys, abrupt withdrawel, fever • AR: anticholernergic effects, psychiatric disturbances, taccycardia • Inter: CNS depressants, alcohol,anticonvulsants, coffee • Pres:2mg 5mg CSHALDERS/GOIT/2008
Parkinsons • Benztropine mesylate (Cogentin) • Anticholernergic effects Prec: taccycardia,preg, glaucoma • AR: antichol effects, confusion, tacycardia • Inter: phenothiazines, haleperidol, tricyclic antidepressants CSHALDERS/GOIT/2008
Parkinsons • Benserazide/Levodopa (Madopar) • Adverse reactions • Nausea vomiting drowsiness • Prec: Ph psychosis, depression,. Arrythmias, diabetes, abrupt withdrawel, preg • Inter: opiods • Dose: Madopar 62.5 caps=L50mg/B12.5 CSHALDERS/GOIT/2008
Parkinsons • Bromocriptine • Dopamine agonist • Stimulates dopaminergic receptors • Prec:arrythmias, psychosisa,BF • AR: GI, CNS dist • Inter: phenithiazines, haloperidol, metoclopramides CSHALDERS/GOIT/2008
Parkinsons • Bromocriptine is best used in conjunction with levodopa • Classified as a dopamine agonist • May cause nausea in initial stages CSHALDERS/GOIT/2008
Parkinsons • It is normal for combined therpy to be used in Parkinsons disease, however we need to be mindful of polypharmacy in this group CSHALDERS/GOIT/2008
Alzheimers Disease • Primarily a form of dementia, characterised by brain shrinkage, enlarged ventricles • Progressive deterioration of intellectual and cognitive functioning. • First signs forgetful, then confused, and later demented CSHALDERS/GOIT/2008
Alzheimers Disease • Reduction in levels of acetycholine and acetylcholinesterase occurs early in the disease • Evidence also suggests glutamate in the neurodegeneration underlying Alzheimers • Glutamate levels have been found to be raised CSHALDERS/GOIT/2008
Alzheimers disease • The acetylcholinesterase inhibitors rivastigmine,galatamine, donepezil usedin the treatment of mild to moderate alzheimers • Rationale for therapy by blocking the degenerative enzyme for acetylcholine more transmitter will be available and its action prolonged CSHALDERS/GOIT/2008
Alzheimers disease • Donepezil and riastigmine produce a number of adverse effects • Nausea, vomiting elevated liver enzymes, diarrhoea dizziness anorexia • Common adverse effects may be severe enough to stop drug therapy CSHALDERS/GOIT/2008
Alzheimers disease • Donepezil • Requires once day administration • Half life approx 70 hours • Generally well tolerated CSHALDERS/GOIT/2008
Alzheimers disease • Galantamine can cause Gi upset, weight loss anorexia, CNS disturbance, urinary tract infection and fatigue CSHALDERS/GOIT/2008
Alzheimers disease • Memantine • Management of moderate disease • Is an N- Methyl D asparate receptor antagonist that selectively restores the ungated receptors to the gated state and inhibits prolonged calcium ion influx without affecting normal glutamate neurotransmission CSHALDERS/GOIT/2008
Alzheimers disease • Memantine • Is excreted unchanged in the urine contraindicated in people with renal failure • Can make clients feel agitated insomnia drowsiness dizziness headache GIT disturbances CSHALDERS/GOIT/2008
Alzheimers disease • These drugs do not effect the underlying pathophysiological process but when effective do halt the disease for up to two years CSHALDERS/GOIT/2008
Huntingtons Disease • Huntingtons chorea genetic disease characterized by involuntary muscle movements and dementia • Autosomal dominant condition • Uncontrollable muscle movements, lack of coordination clumsiness and short term memory loss • Loss of speech and swallowing and death CSHALDERS/GOIT/2008
Huntingtons Disease • The synthesis of the brain protein called huntington is abnormal • The abnormal huntington accumulates leading to cell death CSHALDERS/GOIT/2008
Huntingtons Disease • Tetrabenazine • Acts by inhibiting the storage of dopamine thus decreasing dopamine activity • Adverse effects • Drowsiness, depression impaired alertness CSHALDERS/GOIT/2008
Huntingtons Disease • Clinical considerations • Do not take with alcohol • Stop if dysphagia occurs • Depression occurs reduce dose CSHALDERS/GOIT/2008
Motor Neuron Disease • Symptoms include muscle fasciculation, hypotonia, muscle wasting • Treatment is to relieve symptoms • No cure and death follows CSHALDERS/GOIT/2008
Motor Neuron Disease • Riluzole • Inhibits the release of glutamate into the neurones, leading to a slowing down of the paralysis • A/E nausea and decreased lung function CSHALDERS/GOIT/2008
Motor Neuron Disease • Supportive Therapy • Tryciclic antidepressants • Oxygen therapy • Antimuscarinics to reduce dribbling • Baclofen and diazepam for spasticity CSHALDERS/GOIT/2008
Nervous system • Sedatives and hypnotics are drugs which depress the CNS by inhibiting transmission of nerve impulses • Classified based on the degree of CNS depression they produce • Sedatives are agents which produces a diminished responsiveness to stimuli without producing sleep • Hypnotics have a more intense depressant effect and usually produce sleep CSHALDERS/GOIT/2008
Benzodiazepines • Most have the suffix azepam • Are thought to have there effects of the neurotransmitter GABA • Long acting are used as anticonvulsants • Medium acting and short acting are used for sleep • Very short are used for anesthesia CSHALDERS/GOIT/2008
Benzodiazepines • Used widely in the treatment of anxiety • Also used as anaesthetics, sedatives and hypnotics and anti anxiety agents. • Whether they are used as hypnotics or sedatives depends on the duration of their action in the body. CSHALDERS/GOIT/2008
Benzodiazepines • BZ1 receptors are found mainly in the cerebellum and are related to anxiety and sedation • BZ2 receptors are found mainly in the basal ganglia and hippocampus and are assoc with muscle relaxation, as well as memory and learning. CSHALDERS/GOIT/2008