Download
1 / 32
320 likes | 335 Views
Explore how lysosomes in hepatocytes handle residues, including lipofuscins and environmental melanosis, impacting liver health. Learn about handling insoluble residues and storage diseases affecting hepatocytes.

E N D
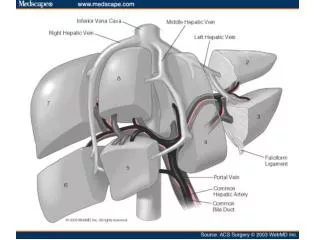
Module 2 OTHER HEPATOCELLULAR DEGENERATIONS Handling the rubbish… lysosomal function in hepatocytes Ideally, unwanted substances are transformed into solutes for excretion, since solutions can usually be excreted easily in bile and urine. But sometimes the end result of these transformations are dense heterogeneous polymers that resist further breakdown. Such residues would interfere with hepatocyte function if they remained free in the cytoplasm. Insoluble residues are less harmful if they can be isolated from the general cytosol in membrane-bound bodies (lysosomes). A crude analogy of lysosomal function is that they act like plastic garbage bags, keeping the rubbish out of the way while trying to further degrade it with acid hydrolases, etc.
Module 2 Lysosomes: membrane-bound bodies of varying density Another intoxicated liver. Degenerate hepatocyte cytoplasm being taken up as an autophagolysosome. Also known as cytosegresomes or Councilman bodies. Image courtesy Majid Ghoddusi OTHER HEPATOCELLULAR DEGENERATIONS Handling the rubbish… lysosomal function in hepatocytes These lysosomal residues have 2 basic origins: they can be derived from unwanted ingested compounds (xenobiotics)… …or they can be the end result of autophagy, when damaged organelles end up in lysosomes (autophagolysosomes). Lipofuscins are common components of lysosomal residues. They are produced when damaged or redundant organelle membranes are processed in autophagolysosomes.
Module 2 The lysosomal lipofuscin deposits are heaviest in periacinar hepatocytes of this old cat. Environmental melanosis, bovine liver (abattoir specimen) Normal bovine liver (abattoir specimen) OTHER HEPATOCELLULAR DEGENERATIONS Handling the rubbish… lysosomal function in hepatocytes Over time, lipofuscins accumulate in lysosomes of older hepatocytes, Kupffer cells and portal lymph node macrophages. They impart a brownish colour to the tissues Hepatic environmental melanosis is another example of a lysosomal residue problem. Most individuals in a flock (usually sheep, sometimes cattle) on a particular pasture may have livers darkened by melanin. The melanin is the end result of metabolism of an unknown xenobiotic. It is chemically stable, and persists indefinitely in lysosomes, principally in periportal hepatocytes.
Module 2 Dense lysosomal residues in a Kupffer cell Image courtesy Majid Ghoddusi OTHER HEPATOCELLULAR DEGENERATIONS Handling the rubbish… lysosomal function in hepatocytes Insoluble lysosomal residues can be eliminated from hepatocytes by 2 processes. They may be expelled into the bile canaliculus in particulate form (lysosomes tend to be more common in pericanalicular cytoplasm), or they may be shed into Disses space when the host hepatocytes dies or regurgitates them. From here, they may be taken up by Kupffer cells, or reach local lymph nodes. In individuals with heritable deficiency of a lysosomal enzyme, the substrate of the absent enzyme tends to accumulate within lysosomes. These so-called “storage diseases” have their most significant effects on the longest-lived, most complex cells in the body; ie, neurons Storage diseases also affect hepatocytes, but accumulations tend to be less significant, perhaps because hepatocytes have alternate means of handling the material (and hepatocytes are not as long-lived as neurons).
Module 2 …the “classic” appearance, where the nuclear chromatin is displaced to lie against the nuclear membrane, with the inclusion (which tends to be more basophilic than eosinophilic) situated centrally in a clear space… OTHER HEPATOCELLULAR DEGENERATIONS Intranuclear inclusions in hepatocytes In most people’s minds, intranuclear inclusions implicate virus infections. While this is more likely to be true in other tissues, in liver there are several other types of I/N inclusion have no viral association. Most are not associated with clinical disease, and are incidental findings during necropsy histopathology. First, the viral intranuclear inclusions… The classic example is the amphophilic I/N inclusion seen in infectious canine hepatitis (canine adenovirus 1) infection. Not all cases of ICH show good hepatocyte I/N inclusions, but when present, they take at least two forms… …and the “collapsed” form (probably a later stage), where the nuclear membrane has collapsed as if punctured, and is draped over the inclusion. (images courtesy P. Pesavento; U.C.Davis)
Module 2 Generalised canine herpesvirus infection (image courtesy P. Pesavento; U.C.Davis) OTHER HEPATOCELLULAR DEGENERATIONS Intranuclear inclusions in hepatocytes (contd.) Herpesvirus hepatitis is also characterised by intranuclear inclusions in hepatocytes in many species. These inclusions are usually more eosinophilic than those of the adenoviruses, but otherwise their morphological features can be very similar. A smaller proportion of cases of herpetic hepatitis show convincing I/N inclusions than do cases of adenovirus hepatitis (in dogs, at least). Some believe that they are better demonstrated in material that is (a) fresh, and (b) has been fixed in an acid fixative. Be that as it may, one shouldn’t rely on the presence or absence of these inclusions to confirm or rule out diagnosis of herpesvirus infection.
Module 2 Bovine liver; suspected pyrrolizidine alkaloid poisoning Intranuclear cytoplasmic invagination; probable location of nuclear pore Cytoplasmic invagination into a hepatocyte nucleus. In the right plane of section in TEMs, the included cytoplasm (complete with organelles) can be seen to maintain continuity via the nuclear pore. OTHER HEPATOCELLULAR DEGENERATIONS Intranuclear inclusions in hepatocytes (contd.) The hepatocyte nucleus can sometimes engulf adjacent cytoplasm, along with a few organelles. In ordinary sections, the nucleus seems to have a hollow spherical vesicle inside: the cytoplasmic nature of the inclusion is not apparent. The true nature of these engulfments or invaginations is only revealed by transmission electron microscopy. This phenomenon is rare in healthy livers, but can be quite a feature of chronically intoxicated hepatocytes. To what extent it is reversible, or threatening to the survival or function of the hepatocyte, is unknown.
Module 2 OTHER HEPATOCELLULAR DEGENERATIONS Intranuclear inclusions in hepatocytes (contd.) In some species, lead (Pb) intoxication can lead to the development of intranuclear inclusions in hepatocytes and renal proximal tubular epithelium. Their occurrence is probably more common in the kidney than the liver. These inclusions are very electron dense: not surprising, since they consist of lead in combination with an organic matrix. They are also acid-fast with the standard Ziehl-Neelson stain, which is handy for diagnostic purposes. It seems the nucleus can handle a bit of garbage disposal. Very democratic of it, considering its more executive duties.
Module 2 Older koalas often have prominent amphophilic inclusions in their hepatocyte nuclei. OTHER HEPATOCELLULAR DEGENERATIONS Intranuclear inclusions in hepatocytes (contd.) Another intranuclear inclusion is the crystalline type with a sharply rectangular profile, most often seen in canine hepatocytes of older animals. It is intensely eosinophilic and may cause the nuclear membrane to be stretched around it. Electron microscopy has shown these bodies to be composed of a regular lattice of electron-dense components. They have nothing to do with heavy metal intoxication (see Pb poisoning, above). There is no known cause or association. They are just enigmatic incidental findings Neither histochemistry nor transmission electron microscopy has revealed anything useful about them: they seem to consist of amorphous relatively electron-dense sludge. Again, there is no apparent relationship to other disease conditions. (The pigment granules are normally found in older koalas’ hepatocyte cytoplasm. We know nothing about them, either.)
Module 2 Marked biliary hyperplasia secondary to chronic extrahepatic biliary obstruction (cholelithiasis) in a horse. BILIARY HYPERPLASIA Hepatic stem cells (progenitor cells) are bipotential cells capable of differentiating into either hepatocytes or cholangiolar epithelial cells (i.e. bile ductules). The stimulus for proliferation of hepatic stem cells may be loss of hepatocytes (e.g. due to periacinar necrosis), injury to biliary epithelium or prolonged cholestasis. In many situations, biliary hyperplasia appears to be an attempt to regenerate lost parenchyma. The most common manifestation of stem cell proliferation is formation of bile ductules, also referred to as “biliary hyperplasia” or “cholangiolar hyperplasia”.
Module 2 Image courtesy National Toxicology Program OVAL CELL HYPERPLASIA Oval cells are regarded as a subset of hepatic stem cells, or facultative stem cells. They are thought to arise from cells that line terminal bile ductules (canals of Hering). Oval cell hyperplasia is characterised by periportal proliferation of cells with oval shaped nuclei and scant cytoplasm, with minimal formation of tubular structures. Oval cell hyperplasia is a much less common manifestation of stem cell proliferation than biliary hyperplasia. Oval cell hyperplasia Extensive oval cell proliferation is a characteristic response of the rodent liver. Similar responses are reported only rarely in domestic animals (or humans). Oval cell hyperplasia can occur independently or be associated with conventional biliary hyperplasia. Biliary hyperplasia Binucleated hepatocytes may also be a feature of hyperplasia, especially in some species (e.g. rodents).
Module 2 AMYLOIDOSIS Amyloid is a proteinaceous substance, with a β-pleated structure, which is deposited extracellularly. In the liver, is mainly AA (secondary or reactive) amyloid, which is derived from serum amyloid A. The latter is synthesised by hepatocytes, classically associated with systemic inflammatory conditions, though the latter cannot always be identified. It is less frequently AL (primary) amyloid derived from immunoglobulin light chains, that is usually associated with neoplasia of plasma cells.
Amyloid is initially deposited in the space of Disse. As amyloid accumulates, it causes pressure atrophy of hepatocytes. AMYLOIDOSIS is an infiltrative process.
Module 2 DESCRIBING HEPATOCYTE NECROSIS • Based on individual cell morphological changes • Apoptosis • Oncosis • Based on the mass of necrotic cells • Coagulative necrosis • Liquefactive (lytic) necrosis • Caseous necrosis • Based on the distribution of necrosis • Focal necrosis (randomly distributed) • Periacinar (centrilobular) necrosis • Midzonal necrosis • Periportal necrosis • Massive necrosis • Piecemeal necrosis • Necrosis of sinusoidal lining cells • Necrosis of bile duct epithelium
Module 2 NECROSIS Necrosis is traditionally defined as the death of cells in living tissue. It also refers to the morphologic changes that follow cell death. There are two major types of cell death: (a) preceded by cell shrinkage (apoptosis) (b)preceded by cell swelling (the term oncosis has been proposed to describe this). In current literature, necrosis is used in one of two ways: (a) broadly, to describe the process of cell death in liver tissue and the associated morphologic changes, regardless of the pathway by which the cells died. (b)in a more narrow sense,to describe cell death occurring by non-apoptotic pathways (e.g. oncosis). This approach tends to oversimplify a dichotomy between apoptosis and “necrosis”.
Module 2 Apoptotic body, taken up by hepatocyte APOPTOSIS Is one form of cell death and is characterised by cell shrinkage while dying. The cell dies in an orderly (“programmed”) fashion without loss of integrity of the cell membrane. Apoptosis requires continued ATP and protein synthesis, and energy continues to be used by the affected cell. Apoptosis is characterised by nuclear chromatin condensation, margination, and fragmentation, with cleavage of DNA into regularly sized fragments. Usually (though not always) it affects individual isolated cells in a tissue rather than groups of contiguous cells. The apoptotic cell undergoes fragmentation to produce membrane-bound apoptotic bodies. These are rapidly phagocytosed (within a few hours) by neighbouring parenchymal cells or macrophages (Kupffer cells). Apoptotic cells may also be identified using immunohistochemical stains (e.g. activated caspase-3 and TUNEL).
Module 2 Comparison of apoptotic necrosis with oncotic necrosis Apoptotic bodies are phagocytosed. No inflammatory response Further shrinkage, membrane-bound fragments flung off Apoptosis begins (cell shrinks, chromatin condenses) Viable cell Oncotic necrosis. Cell components escape and trigger inflammatory response Cell membrane becomes leaky, “blebbing” Hydropic degeneration (cell swells but still alive)
Module 2 In this case of zonal necrosis (presumably toxic) in sheep liver, these fragments could be the end result of necrosis, or of intense apoptotic activity. Special techniques (TEM; immunohistochemistry) are needed to distinguish the processes (which of course may occur concurrently). APOPTOSIS The death of a cell by apoptosis is a very tidy business. Very little tissue distortion results, since typically only one cell at a time is removed and so no gaping defects are left. Apart from the mopping up by macrophages, there is little or no inflammatory response. If the apoptotic bodies contain condensed basophilic nuclear remnants, they are more easily recognised. Such fragments may be confused with pyknotic remnants of nuclei resulting from non-apoptotic cell death. Apoptosis in the liver is usually the mechanism by which individual senescent or terminally damaged hepatocytes are removed. So sometimes it is a normal event in the cell’s life-cycle, and sometimes a part of a pathological process. The term necrobiosis has been used to describe the physiological death of individual senescent cells in any tissue (usually by apoptosis), this being a normal event in the constant turnover of cell populations. Note however that this term “necrobiosis” has also been used to describe degeneration of collagen bundles in the dermis, and to a large extent it has fallen out of use.
Module 2 NECROSIS In these modules, we use the term necrosis broadly for the histologic changes that occur following cell death by either pathway (apoptosis or necrosis), using apoptotic necrosis or oncotic necrosis when a distinction needs to be made. This is in keeping with the traditional definition of necrosis as death of cells in living tissue, which applies equally well to cells having died via apoptosis or oncosis. Both forms of cell death (apoptosis and oncosis) may be caused by the one agent and may coexist in the one tissue. To some extent the severity of the insult may determine whether cells die by apoptosis or oncosis. “Degeneration” is an appropriate term when there is uncertainty that the observed cells are actually dead.
Module 2 NON-APOPTOTIC CELL DEATH (ONCOTIC NECROSIS) Non-apoptotic cell death may affect isolated individual cells or groups of contiguous cells. It is preceded by cell swelling (hydropic degeneration) which then becomes irreversible. Uncontrolled fluxes of water and solutes, combined with loss of membrane integrity, results in the cell bursting. The morphologic appearance of necrosis is the result of one or both of two processes: (a) denaturation of intracellular proteins (b) enzymatic digestion of the cell. The enzymes may originate from lysosomes of the dead cell, infiltrating leucocytes or bacteria. Nuclear changes may include one or more of pyknosis, karyorrhexis, karyolysis or absence of nuclei. Once the necrotic cells have undergone these early alterations, the mass of necrotic cells may have one of several morphologic appearances ….
Module 2 Zone of coagulative necrosis; presumably more rapid death. Zone of lytic necrosis; hepatocyte remnants “washed away” and replaced by blood. Surviving (but distressed; fatty change) periportal hepatocytes. APPEARANCE OF THE MASS OF NECROTIC CELLS When rapid denaturation of cytoplasmic proteins (including enzymes) predominates, coagulative necrosis develops. Proteolysis is delayed and the dead cells remain recognisable, retaining their basic outline. The general tissue architecture is preserved. The cytoplasm usually stains with increased eosinophilia. When rapid enzymatic digestion predominates, lytic (liquefactive) necrosis develops, with disintegration and loss of the cell, accumulation of cell debris and possibly replacement haemorrhage. Caseous necrosis implies conversion of dead cells into a granular friable mass grossly resembling cottage cheese. It implies an older, chronic lesion and the tissue architecture is completely obliterated. It more commonly used to describe a gross rather than histologic appearance. Coagulative and lytic necrosis can be caused by the same insult, and the differences may relate more to the tempo of the process than to anything else. While it is convenient to classify necrotic lesions as coagulative, lytic or caseous, it does not always accurately reflect the complexity of what has happened. Some necrotic lesions cannot be neatly classified using these terms.
Module 2 Rabbit liver; salmonellosis Focal hepatitis involving liquefactive necrosis of hepatocytes. NECROSIS Non-zonal distribution of hepatocellular necrosis The term focal necrosis is used when there are isolated groups of dead hepatocytes that are randomly distributed with respect to acinar zones, and there is no discernible zonal pattern to the distribution. Focal necrosis is most often caused by something that has been removed from sinusoidal blood by a Kupffer cell. More often than not this is an infectious agent. This is not surprising when one considers the frequency with which microbes and other particles travel from the gut to the liver in the portal blood. Hepatocytes themselves may be involved in the infection, or they may simply be destroyed as “innocent bystanders”. There is usually more accompanying inflammation than there is with zonal necrosis, so in many cases there may be argument as to whether the process should be called focal necrosis or focal hepatitis. Those who don't like arguing can fudge the issue by describing it as “focal necrotising hepatitis”.
Module 2 These are apoptotic bodies, now taken up by macrophages after apoptotic death of hepatocytes. NECROSIS Single cell necrosis It is more important to try to distinguish between necrosis of groups of hepatocytes, and death of isolated hepatocytes (single cell necrosis). Sometimes hepatocyte necrosis is characterised by the death of isolated individual hepatocytes, rather than in groups. It may occur by apoptosis or may be preceded by cell swelling (oncosis). Single cell necrosis may have a random distribution or (less often) it may have a zonal distribution.
Module 2 NECROSIS Zonal hepatocellular necrosis: periacinar necrosis Zonal necrosis is sub-classified into periacinar, mid-zonal and periportal, according to the distribution of the necrotic hepatocytes within the acinus (see Module 1). Reference back to the acinar structure of the liver (Module 1) reminds us of the special vulnerability of periacinar hepatocytes. Not only are they last to access oxygen and nutrients from sinusoidal blood, but ( with some notable exceptions), they are more susceptible to toxic injury. The reasons for this are discussed in Module 4 (hepatoxicities) An important question: are the morphological features of the necrosis caused by these insults sufficiently different to enable us to differentiate between them histologically? Answer: unhappily not. The following 2 images (one from a pig; the other from a cow) are both good examples of periacinar hepatocellular necrosis. One was a case of acute hepatoxicity; the other was a case of severe acute haemorrhagic anaemia… can you tell you which is which?
Module 2 Pig liver; periacinar necrosis. Bovine liver; periacinar necrosis. Portal triad Hepatic venule. NECROSIS Zonal hepatocellular necrosis: periacinar necrosis The only real difference is that there are scattered inflammatory cells associated with the necrotic cells in the pig. This has more to do with how long the cells have been dead, than with the cause of the necrosis. The cow had recently consumed a toxic dose of Cestrum parqui, while the pig had bled to death from a gastric ulcer. But there’s no feature of the histopathology that enables you to deduce this. Periacinar necrosis is by far the most common form of zonal liver necrosis. This is hardly surprising, since it is often seen in animals that have died slowly with progressive circulatory failure (circulatory shock); a common final fate. So periacinar necrosis must always be interpreted with caution, especially if present to a minor degree, since it is so often an insignificant agonal phenomenon (see Agonal changes).
Module 2 Peracute massive liver necrosis; cyanobacterial (blue-green algal poisoning); sheep. NECROSIS Zonal hepatocellular necrosis: massive necrosis The term massive necrosis is used when all hepatocytes in contiguous acini have undergone necrosis. This is most commonly seen in very severe liver injury, caused by insults that usually produce zonal necrosis. In fact, in most cases where massive necrosis is the principal feature, one can usually find slightly less severely affected parts of the liver in which the pattern of necrosis is zonal. So massive necrosis may be regarded as the severest possible manifestation of zonal necrosis. However, massive necrosis may also be caused by a vascular disaster involving a large portion of liver, or by the action of necrotising microbes (eg clostridial necrotic hepatitis). In these latter conditions the liver will be asymmetrically affected and this will be obvious grossly.
Module 2 Midzonal necrosis; donkey. History of access to Myoporum laetum. (Ngaio tree). Portal triad (note early reaction of stem cells) Hepatic venule (image courtesy Lucy Anthenill) NECROSIS Zonal hepatocellular necrosis: midzonal necrosis Only rarely do midzonal hepatocytes undergo necrosis, leaving periacinar and periportal hepatocytes more or less intact. The only known causes are certain hepatotoxins. The zonal distribution of the necrosis in such cases is often quite variable, so involvement of any of the 3 acinar zones may be seen in the same outbreak, or even in the same liver. An attempt will be made in Module 4 to explain the mobility of the zone of necrosis produced by these toxins.
Module 2 Periportal necrosis: rabbit liver, calicivirus infection. Periportal necrosis: cow. “Acute bovine liver disease” (ABLD). Hepatic venule Portal triad Periportal and midzonal haemorrhagic necrosis Hepatic venule Portal triad NECROSIS Zonal hepatocellular necrosis: periportal necrosis We have seen that periportal necrosis might be expected as well as midzonal necrosis in some individuals in field outbreaks of Myoporum poisoning. But there are a few examples of liver necrosis that are consistently periportal in distribution. One of these is infectious: the acute haemorrhagic periportal necrosis seen in fatal rabbit calicivirus infections. Another is so-called “Acute bovine liver disease” because of its sudden onset and its unknown cause. It’s assumed to be a hepatotoxicity and some outbreaks have been associated with pastures containing Cynosurus echinatus (rough dogstail). In neither of these conditions do we have any idea why the distribution is periportal.
Module 2 Doberman liver; chronic hepatitis. Portal and periportal non-suppurative inflammatory infiltrates associated with periportal piecemeal necrosis. NECROSIS Piecemeal necrosis The term piecemeal necrosis implies a form of single-cell necrosis seen in human viral hepatitis. It is characterised by death of hepatocytes at the limiting plate (i.e. at the interface of the parenchyma and connective tissue of the portal tract). The limiting plate is eroded in a piecemeal fashion. Piecemeal necrosis is accompanied by a variable degree of mononuclear inflammation, which tends to obscure the edge of the portal tract and interweave amongst periportal hepatocytes, often encircling single or small groups of hepatocytes. Piecemeal necrosis is a defining feature of so-called “chronic active hepatitis” of humans (now called interface hepatitis). Rightly or wrongly, in veterinary pathology the terms “piecemeal necrosis” and “chronic active hepatitis” have been applied to the single-cell necrosis and mononuclear infiltration that is most obvious adjacent to portal tracts, particularly in Dobermans. It is assumed to be immune mediated and is better simply called chronic hepatitis.
Module 2 Normal avian liver, perfusion-fixed. Kupffer cell Endothelial cell Lytic necrosis of sinusoidal-lining cells 12 hr after oral monocrotaline dosage; (broiler chicken). (hepatocytes are relatively unscathed) (image courtesy Majid Ghoddusi) (image courtesy Majid Ghoddusi) NECROSIS Necrosis of sinusoidal lining cells • Necrosis of sinusoidal lining cells may occur early in the course of other acute hepatotoxicities (e.g. acetaminophen poisoning). • presumably this is a result of spillover of toxic metabolite or parent compound from hepatocyte cytoplasm into the space of Disse. • In addition, certain toxins appear to selectively injure hepatic sinusoidal endothelial cells. • for example, microcystin-LR produced by Microcystis aeruginosa, a cyanobacterium (blue-green alga) • and the pyrrolizidine alkaloid monocrotaline can destroy endothelial cells in chickens while leaving hepatocytes alive. Necrosis of sinusoidal endothelial cells may lead to significant haemorrhage within areas of necrosis. Sinusoidal macrophages (Kupffer cells) may undergo necrosis as a result of their role in clearing portal blood of particulate material (should these particles be toxic or infectious). While Kupffer cell necrosis may occur alone, more usually there is also damage to surrounding hepatocytes.
Module 2 NECROSIS Necrosis of biliary epithelium Selective necrosis of biliary epithelium is unusual but is seen in a number of situations, usually accompanied by at least some degree of portal inflammation. Some causes: • some experimental compounds (e.g α-naphthylisothiocyanate). • sporidesmin poisoning (facial eczema) (see chronic hepatotoxicities, Module 4). There is necrosis and loss of biliary epithelium with peribiliary oedema or fibrosis and usually minor inflammation. • idiosyncratic drug-induced liver injury. There may also be loss of bile ducts (“vanishing bile duct syndrome”). Trimethoprim sulpha has been implicated in dogs.
Module 2 LIVER PATHOLOGY Module 3 follows: • Module 1 • Background, normal structure, developmental anomalies • Functions of the liver • Failure of function (including clinical chemistry) • Module 2 • Consequences of liver size • Sampling (including normal cytology) • General pathological reactions • Necrosis • Module 3 • Inflammation • Circulatory disturbances • Final common pathway of chronic liver disease, incl. fibrosis • Viral infections • Module 4 • Bacterial infections • Parasitic infections • Acute hepatotoxicities • Chronic hepatotoxicities • Neoplasia