Download
1 / 22
260 likes | 509 Views
Acute Lymphoblastic Leukemia. Maggie Davis Hovda 5/26/2009. Definition. Neoplastic disease which results from a mutation in a single lymphoid progenitor cell at one of several discrete stages of development B Cell or T Cell. Epidemiology. Most common childhood acute leukemia, ~80%

E N D
Acute Lymphoblastic Leukemia Maggie Davis Hovda 5/26/2009
Definition • Neoplastic disease which results from a mutation in a single lymphoid progenitor cell at one of several discrete stages of development • B Cell or T Cell
Epidemiology • Most common childhood acute leukemia, ~80% • Incidence in adults ~20% • Bimodal distribution of occurrence: • Peak at age 2-5 • Second increased incidence after age 50
Pathogenesis • Acquired Genetic Change in Chromosome • Change in number, ie ploidy • Change in structure • Translocations (most common) • Inversions • Deletions • Point mutations • Amplifications Changes in normal means of cell differentiation, proliferation, and survival
1 – Activation of a proto-oncogene OR creation of a fusion gene with oncogenic properties - Ph Chromosome t(9;22) 2 – Loss or inactivation of ≥ 1 tumor suppressor gene - p53 (p16 mutation) Mechanisms of Leukemia Induction
Etiology • Unknown • ? Genetic Predisposition • Increased incidence amongst monozygotic and dizygotic twins • Down Syndrome • Disorder with chromosomal fragility: • Fanconi’s anemia • Bloom Syndrome • Ataxia-Telangiectasia • ? Infections • HTLV1 in T cell leukemia/lymphoma • EBV in mature B cell ALL • HIV in lymphoproliferative DO
Presentation • Nonspecific Symptoms • Fatigue/decreased energy • Fever • Easy bruising • Bleeding • Dyspnea • Dizziness • Infection • Joint, extremity pains • CNS involvement
Physical Exam Pallor Ecchymoses Petechiae LAD Hepatosplenomegaly Lab Abnormalities anemia wbc vary 0.1 (20-40%) - >100 k (10-16%) Platelets – usually ↓ ↑ LD, uric acid CXR: eval for thymic mass CSF to eval for involvement Clinical Presentation
Diagnosis • Morphologic • French American British Classification • L1: small uniform blasts (pediatric ALL) • L2: larger, more variable sized blasts (adult ALL) • L3: uniform cells with basophilic and sometimes vacuolated cytoplasm (mature B cell ALL)
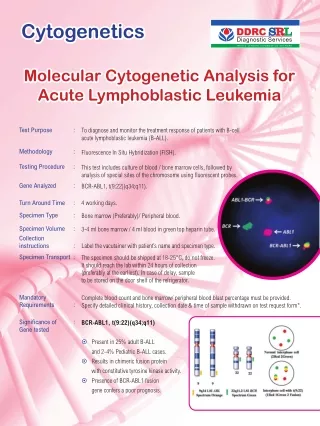
Immunophenotyping From: Jabbour, E. et al. Adult Acute Lymphoblastic Leukemia. Mayo Clinic Proc. 2005;80(11):1517-1527
Cytogenetic Abnormalities From: Jabbour, E. et al. Adult Acute Lymphoblastic Leukemia. Mayo Clinic Proc. 2005;80(11):1517-1527
Classification of ALL From: Harrison’s Principles of Internal Medicine, 16th ed. 2005. Chapter 97, Malignancies of lymphoid cells.
Differential Diagnosis • ITP • Aplastic Anemia • Infectious mononucleosis • Rheumatoid Arthritis • Rheumatic Fever • Collagen Vascular Disease
Treatment • 1 – Remission Induction • 2 – Intensification (Consolidation) Therapy • 3 – Maintenance Therapy • 4 – CNS Prophylaxis • 5 – Allogeneic Stem Cell Transplant
Treatment • Remission Induction • Goals: restore normal hematopoiesis, induce a complete remission rapidly in order to prevent resistance to drugs • Standard induction regimen • 4 or 5 drugs: vincristine, prednisone, anthracycline, L-asparaginase, +/- cyclophosphamide • Intensification • High doses of multiple agents not used during induction or re-administration of the induction regimen
Treatment • Maintenance Therapy • Daily po 6MP, weekly MTX, monthly pulses of vincristine and prednisone for 2-3 yrs • CNS Prophylaxis • Given during induction and intensification • Intrathecal: MTX, Cytarabine, corticosteroids • Systemic: high dose mtx, cytarabine, L-asparaginase • +/- Cranial Irradiation
Treatment • Stem Cell Transplant • Done during first CR • Indications: • Ph Chromosome • t(4;11) mutation • Poor initial response to induction therapy • Other • Adolescents benefit significantly from pediatric ALL regimens vs. adult regimens
Relapse & Prognosis • Relapse • Most occur during treatment or within the first 2 years • Bone Marrow is the most common site • Poor prognostic factors in patients previously treated: • Relapse on therapy • Short initial remission after intense therapy • T-cell immunophenotype • Ph Chromosome • Circulating blasts • High leukocyte count at relapse
Prognosis • Overall better in children than in adults • In adults, worse outcomes with: • Increasing age, >60 • Increased wbc count at presentation
Sources • Jabbour, E. et al. Adult Acute Lymphoblastic Leukemia. Mayo Clinic Proc. 2005;80(11):1517-1527 • Xavier, T. Chemotherapy of acute leukemia in adults. Expert Opin. Pharmacother. (2009) 10(2):221-237 • Williams Hematology, 6th ed. 2001. Chapter 97, Acute Lymphoblastic Leukemia. • Harrison’s Principles of Internal Medicine, 16th ed. 2005. Chapter 97, Malignancies of lymphoid cells.