Download
1 / 41
460 likes | 1.07k Views
STATUS EPILEPTICUS UPDATE. Jo Wilmshurst Department of Paediatric Neurology Red Cross Children’s Hospital. What are the protocols? How should we monitor these children?. Definitions. Status epilepticus: Generalised convulsions > 30 minutes = brain damage / neuronal cell death

E N D
STATUS EPILEPTICUS UPDATE Jo Wilmshurst Department of Paediatric Neurology Red Cross Children’s Hospital
What are the protocols? • How should we monitor these children?
Definitions • Status epilepticus: Generalised convulsions > 30 minutes = brain damage / neuronal cell death • Refractory status: Generalised convulsions > 1hour, resistant to level 1-2/3 intervention – i.e. need PICU intervention • The longer it takes to gain control the worse the outcome and the harder it will be to terminate Sz • Outcome influenced by underlying aetiology – encephalitis worst result Scott et al, ARCH 1998 Holtkamp et al; JNNP 2005
Causes • Fever 36% • Medication change 20% • Unknown 9% • Metabolic 8% • Congenital 7% • Anoxic 5% • Other (trauma, vascular, infection, tumour, drugs) 15% Haafiz et al; Ped Emerg Care 1999
Mortality • Adults 15-22% • Children 3-32% • No figures for SA Fountain et al; Epilepsia 2000 Lacroix et al; CCM 1994 Sahin et al; Epilepsia 2001
Optimal intervention times • Children > 5 years : typical GTCS seizure duration < 5 minutes • Younger children and infants: paucity of data. Suggested time frame for a typical GTCS is less than 10-15 minutes. • Mean age for status in children 3.4 years Lowenstein DH, Bleck T, Macdonald RL. Epilepsia 1999;40(1):120-2 Singh et al 2010 Neurology
Diagnostic assessment of the child with status epilepticus • Blood glucose • Anti-epileptic drug (AED) levels. • Toxicology testing • Blood cultures • Lumbar puncture • (as clinically indicated & all children < 18 months) • Neuroimaging: • Insufficient evidence for routine neuroimaging (8% yield) Indications: • When convulsive status is unexplained • the patient remains unconscious, • or new focal neurological signs become apparent. Evidence- based quideline American Academy of Neurology (ANN) and Child Neurology Society (CNS)
Brain Monitoring • Continuous • Non-invasive • Highly sensitive to a variety of brain insults • Reasonably specific • User friendly • Not too expensive! Kurtz et al Curr Opin Crit Care 2009
Monitoring cEEG (continuous EEG – full head montage) • The Gold standard – not viable in most SA settings • Non-convulsive seizures • Ischaemia aEEG (Amplitude-integrated EEG) • Assessing if burst suppression attained • Non-convulsive seizures • Potential artefact • Need to remember overall underlying cause usually the defining feature for the outcome of the child.
The future? • Basic external monitoring (BP, sats, HR) often underestimates true cerebral function • Cerebral Near-infrared spectroscopy (cNIRS) • Non-invasive • Used as a tool to assess regional brain saturations (RSO2) • Available in SA! • Comparison studies with serological markers (S100beta and NSE) – performed well (better infact) Subbaswamy et al Neurocrit Care 2009
Treatment of Status Epilepticus • Pre hospital treatment • A&E treatment • In-hospital treatment (Ward/High care) • Anaesthesia (ICU)
What recommendations exist for managing Status Epilepticus in Children?
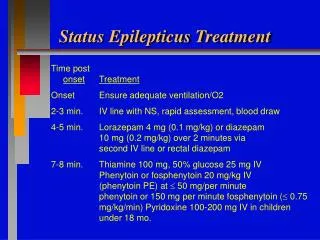
APLS guidelines (2005; The convulsing child) ABCD ↓ (Level 1) Lorazepam IV/IO or diazepampr / midazolam buccal ↓ Lorazepam IV / IO ↓ Paraldehyde pr (Level 2) ↓ Phenytoin IV / IO / Phenobarbitone IV / IO ↓ (Level 3) RSI with Thiopental
Level one • Arrival – First Hosp intervention • Benzodiazepine • Diazepam PR/IV/IO • Midazolam IN/SL/IV/IO • Lorazepam IV/PR/IO • Repeat if necessary • Good specialist consistency, good study data Scott et al;Lancet 1999 Jeannet et al;Europ J Paed Neurol 1999 DeNegri et al; Pediatr Drugs 2001
Diazepam versus Lorazepam • Both are equally effective at aborting status epilepticus. • IV lorazepam vs IV diazepam • Rectal lorazepam might be more effective than rectal diazepam • Lorazepam: • Substantial longer duration of anti-seizure activity (lipid-soluble) • Less seizure recurrence and fever repeat doses required. Appleton R et al Cochrane Database Syst Rev 2008 Jul 16;(3)
Transmucosal pharmacological therapy • Intranasal midazolam as effective as intravenous diazepam • Buccal midazolam as effective as rectal diazepam. • Intravenous formulations of midazolam (given buccal or intranasal routes) are relatively inexpensive. • Caregivers prefer intranasal midazolam to rectal diazepam. Appleton R et al Cochrane Database Syst Rev 2008 Jul 16;(3)
Paraldehyde • Treatment with IV phenytoin as a second-line therapy was associated with a 9-times greater likelihood of seizure termination than was treatment with paraldehyde Chin R, Neville B et al Lancet Neurol 2008;7:696-703
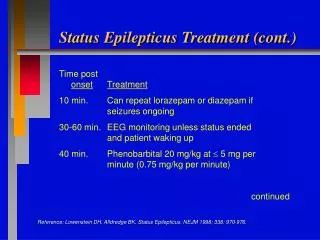
Level 2 intervention • Phenytoin IV • over 20 mins, cardiac monitor, large vein, not mixed with glucose • Phenobarbitone IV/IM • Push, flush through, monitor for resp depression and hypotension • Both agents fairly accepted • BUT studies becoming more limited • small numbers • less children Shanner et al;Neurol 1988 Prasad et al;Ann Neurol 2002
Phenytoin • Takes 30 minutes to administer • Requires a syringe driver • Requires a large IV (NOT central) line • Requires cardiac monitoring for potential cardiac toxicity • Can only be given by IV route • Cannot be repeated • It not as effective as phenobarbitone DeToledo & Ramsay; Drug Saf 2000 Trieman et al; NEJM 1998
Fosphenytoin • More favourable vehicle that does not contain proylene glycol and pH 8.6-9 • Administer in dextrose containing IV solutions at a more rapid rate. • Equally effective: Time for conversion of pro-drug to active drug (8-15minutes) = therapeutic phenytoin concentrations reached at the same time. • Cost: Fosphenytoin 3 times equivalent dose of IV Phenytoin. • Benefit: More favorable side effect profile (purple glove syndrome)
Experimental Rescue therapy • NG phenobarbitone • 20mg/kg given during level 2 intervention • Provided good airway protection and ability for gastric absorption … • Study at Red Cross(Wilmshurst et al J Paed Child Health 2009) • Any child / infant entering established status (Level 2) • 1-4 hours to therapeutic levels • SAFE • No need for repeat dosage for therapeutic levels but for control of seizures could safely repeat • Good viable addition to the protocol – especially where parenteral access or supply lacking Syed et al;Dev Pharmacol Ther 1986 Yska et al;Pharm World Sci 2000 Yukuwa et al;J Clin Pharm Ther 2005
Level 3 intervention • Basically heading into refractory status • Disastrous situation • Resistant seizures – • prob exacerbated by underlying cause ( eg encephalitis), • secondary complications from drugs • hypotension, • respiratory depression • all affecting brain perfusion Sahin et al;Neurol 2003 Scott et al, ARCH 1998 Holtkamp et al; JNNP 2005
Level 3 intervention: Treatment of refractory SE • No prospective randomised trials comparing the effects of anesthetics in the treatment of RSE. • Safety data lacking. Options: • Barbiturate anesthetics: Pentobarbital (US) Thiopental (Europe Aus) • Propofol • Midazolam. • Evidence based medicine: No recommendations on data available. • Even in a large survey of neurologists in USA – little consensus for 3rd / 4th line intervention (J Neurol Sci 2003) Rosenow et al;Epileptic Disord 2002
Midazolam infusion • Requires a syringe driver • Greater risk of airway suppression (especially following previous Benzo boluses) • Takes long time to gain control (range 15 mins – 4.5 hours) • Potential for children left with prolonged seizures and irreversible neuronal cell death in centres without high care facilities • NOTE: Excluded from APLS guidelines Rivera et al; CCM 1993 Lal Koul et al; ARCH 1997 Ozdemir et al; Seizure 2005
CLONAZEPAM INFUSION NO EVIDENCE
Thiopentone • Poor anticonvulsant • Marked haemodynamic effects • Prolonged drug effects if infusion used • Local ICU capacity limited • Staffing • Monitoring • Anaesthetic experience
Very-high-dose Phenobarbitone • Both barbiturates and benzodiazepines exert a primary effect on the GABA receptor complex. • No antiepileptic ceiling effect ! No maximum dose beyond which further doses are likely to be ineffective >200mgkg! Complications: • Sedative and respiratory-depressant properties more likely in combination with benzodiazepines. • Hypotension unusual and related to the highest Phenobarbitone levels and easily controllable. • Complications usually related to underlying aetiology Crawford et al; Neurol 1988
Intravenous Sodium Valproate • FDA approved 1996. • Not in APLS guidelines • No reports of respiratory depression or hypotension. • Caution in children with underlying liver disease or suspected mitochondrial disorder. • Potential hepatic encephalopathy • Comparative studies: • Intravenous Sodium Valproate vs Diazepam infusion • Intravenous Sodium Valproate vs Phenytoin. • No large studies measuring efficacy • Larger paediatric focused studies are needed • Still need syringe driver • Very expensive • Drug of choice: Absence status Limdi et al; Neurology 2005 Rossetti & Bromfield; Neurology 2005 Limbdi N et al Epilepsia 2007 48(3):478-483 Morton L et al Pediatr Neurol 2007;36:81-83 Metha V et al J Child Neuro 2007; 22:1191
IV Levetiracetam • FDA approved adults over 16 yrs since 2006 • Limited data in children (most retrospective case reviews – n=10 and n=32) • Loaded with 25-50mg/kg at level 3 • Effective • Safe • Larger comparison studies needed Kirmani et al Ped Neurol 2009 Abend et al Pediatr Crit Care Med 2009 Gamez-Leyva et al CND Drugs 2009
Mx of status epilepticus in SA • Most centres policy of repeated IV PB boluses • Resulted (anecdotally) dramatic reduction in admissions to PICU and complications of status epilepticus • IV Pb: WHO / IMCI guidelines first line for neonates; 2nd line for infants / children in Mx status
Why is IV phenobarbitone so good for resource poor countries? • Highly effective at controlling status • Safe • Cheap • It can be given by rapid IV bolus • It can be repeated • It can be given by IM route • No need for syringe driver • If control not attained at 1 hour time to arrange transfer to tertiary unit – exceptional situation Crawford et al; Neurol 1988; Wilmshurst & Newton; DMCN 2005 Lee et al;Pediatr Neurol 2005
Overall • Still do not have the ideal solution • Still do not know what this is • Need effective, rapidly acting, easy to administer, cheap agent .. • Watch this space! • Prospective comparison study underway relevant for RLC
Final recommendations 2 targets • Rapid identification of the underlying aetiology • Affects treatment • Affects prognosis • Early initiation towards terminating SE • Decreases morbidity and mortality Recommend • Level 1 – benzodiazepines • Level 2 – phenytoin, phenobarbitone, sodium valproate • Level 3 – “other medications” e.g. levetiracetam and pharmacologic coma induction Abend and Marsh. Curr Treat Options Neurol 2009