Download
1 / 35
430 likes | 844 Views
STATUS EPILEPTICUS. Richard L. Friederich, MD Pediatric Neurology Roseville Kaiser Permanente. Disclosure.

E N D
STATUS EPILEPTICUS Richard L. Friederich, MD Pediatric Neurology Roseville Kaiser Permanente
Disclosure Under the IMQ/CMA Standards for Commercial Support, everyone who is in a position to control the content of an education activity must disclose all relevant financial relationships with any commercial interest. A “commercial interest” includes any proprietary entity producing health care goods or services, with the exemption of non-profit or government organizations and non-health care related companies. A financial relationship is relevant if it pertains to the activity’s content matter including any related health care products or services to be discussed or presented. Dr Rich Friederich, has disclosed that he has no relevant relationships with commercial or industry organizations. The CME Department has reviewed the disclosure information for the planners for this program and they do not have relationships that present a relevant conflict of interest.
Goals • To better understand what status epilepticus is • To better appreciate importance of early intervention in SE • To better appreciate importance of a protocol for treating SE
ED call: • 4 y/o • brought in after a 4 minute GTC sz at home • 1st seizure ever • still post-ictal • ED doc asks for the loading dose of Dilantin What do you tell them?
STATUS EPILEPTICUS -- DEFINITION • Formal: seizure or series of seizures producing a lasting epileptic condition • Informal: seizure activity lasting 30 minutes • nearly all self-limiting seizures cease w/in 5 minutes • Impending status epilepticus: sz > 5 minutes • application: any ongoing seizure activity >5 minutes
STATUS EPILEPTICUS -- EPIDEMIOLOGY • ~100,000 per year in USA • 16% of patients with epilepsy • 1/4 occur in pts < 1 y/o • if sz onset <1 y/o, 70% will have SE • 135-156 per 100,000 per year in <1 y/o
Applications • No absolute need to bolus a seizure which has already ceased • No long term prophylaxis for most 1st time seizures • Exceptions: Initial presentation status epilepticus focal seizure strong (+) FHx
ED call 21 month old presents with a temperature of 104 seizure which lasts 40 minutes stops with a single dose of Ativan because the seizure is prolonged, the ED physician wants to do a CT. “After all, status is unusual with febrile seizures” (?) What are the most common causes of S.E. in children?
STATUS EPILEPTICUS – MOST COMMON CAUSES Children fever 36% med change 20% idiopathic 9% metabolic 8% CNS infection 5% HIE 5% trauma 3% CVA 3% EtOH/drug 2% tumor 1% Adults CVA 25% med change 19% EtOH/drug 12% Anoxia 11% Metabolic 9% Idiopathic 8% Fever 5% Trauma 5% Tumor 4% CNS infection 2% DeLorenzo 1992
1st sz - neuroimaging • Neuroimaging suggested for first time seizure • Recommended if SE, focal, or abnl neuro exam • MRI better than CT
You are called to the ED, to await an ambulance responding to a call with a 6 y/o boy with spastic quad CP and his first-ever seizure, which started 25 minutes ago. What is the best treatment to stop the seizures?
In-home treatment • Diazepam given in the home • PR gel form (Diastat) • IV valium given PR or IV • no difference between PR or IV valium • Fosphenytoin given in the home • By extrapolation, other PR meds may be as well • duration SE, duration hosp, incidence of intubation, incidence of sz recurrence in ED • Alldredge, Ped Neuro ‘95 Responsiveness to AED Lowenstein,1993
6 y/o boy with spastic quad CP and his first-ever seizure started 25 minutes ago No meds are given at home You run over your mental check list of the order in which you will approach things. What are the first three things?
A = Airway • B = Breathing • C = Circulation
The patient arrives, still seizing ABC’s are OK Realizing that in a real scenario you will simultaneously approach both the diagnostic and therapeutic aspects: What are the drugs you will try? What are their doses? What is the sequence?
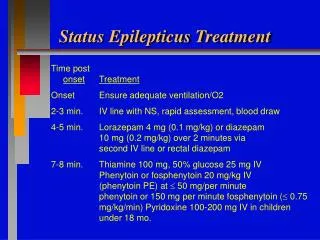
STATUS EPILEPTICUS -- TREATMENT • ABC’s • Quick evaluation • Confirm diagnosis • O2, glucose (+/- 100mg thiamine), [vitamin B6] • treat underlying etiology • Labs: levels, Na, glucose, Ca • Anticonvulsants • Benzodiazepines • Diazepam 0.3 mg/kg (max 10mg) • Lorazepam 0.1 mg/kg (max 4mg) • 20 mg/kg rule • phenobarb • fosphenytoin • valproate • levetiracetam
STATUS EPILEPTICUS – ANTICONVULSANT PROS/CONS Diazepam Rapid efficacy Short effective half life (high fat solubility) Always requires 2nd drug Lorazepam Rapid efficacy Longer half life efficacy Benzodiazepines lose efficacy as SE progresses • Phenytoin adverse effects • Arrhythmias, hypotension • Ppt out in glucose sol’n • Local phlebitis • Cannot give IM • phenytoin may worsen myoclonic szs • Fosphenytoin very expensive • levetiracetam may have neuroprotective effect
STATUS EPILEPTICUS NEUROPHYSIOLOGY • failure of cellular mechanisms to prevent sustained seizure activity • persistent excitation of NMDA receptors • ineffective inhibition at GABA receptors • 2 phases • Activation • Maintenance • Becomes self-sustaining after 15-30 minutes • GABA receptor isoforms change and become ineffective • Phenobarb, benzodiazepines work on GABA
STATUS EPILEPTICUS – ANTICONVULSANT SEQUENCE RATIONALE VA SE Cooperative Study Group NEJM 17Sep98;339(12):792-8 Efficacy GTC SE 384 pts lorazepam 64.9 % phenobarbital 58.2 % diazepam then phenytoin 55.8 % phenytoin 43.6% • Key points • Administer meds early and quickly • Protocol more effective, regardless of sequence (meds given quicker) • Benzos and phenobarb effective early • PHT, VPA, LVT effective later • Midazolam for failure
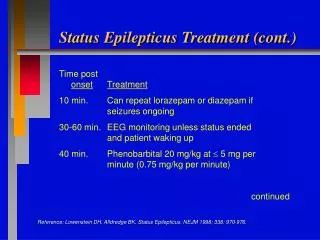
Suggested protocol • Lorazepam 0.1 mg/kg IV or PR • Repeat lorazepam 0.1 mg/kg in 5 minutes (draw up after 3 minutes) • Phenytoin/fosphenytoin 20 mg/kg in 5 minutes • Phenobarb 20 mg/kg in 5 minutes • Phenytoin/fosphenytoin 10mg/kg in 5 minutes
While you are working through your anticonvulsant treatment, what diagnostic work-up are you considering?
STATUS EPILEPTICUS -- EVALUATION • H&P • Blood: ‘lytes, glucose, Ca, BUN, CBC, ABG, LFT, AED level, tox chromatography • Urine: toxicology screen • Febrile: culture blood, urine, CSF; plus CXR • CT or MRI if no etiology or have suspicion
If he fails to respond to initial meds, what else should you think about?
Considerations for SE AED failure • Phenytoin level >35 • CBZ or PHT for primary generalized sz • Symptomatic (glu or Na abnl, drug or med, etc) • <18 m/o: B6 dependency • <6 m/o: Folinic acid responsive epilepsy
Refractory STATUS EPILEPTICUS • Definition: • > 60 minutes, or failed ≥2 anticonvulsants • Rx options: to produce burst suppression EEG • Midazolam • 0.2 mg/kg bolus • then 1-10 g/kg/min • Pentobarb • 15 mg/kg bolus • then 1-5 mg/kg/hr • propofol contraindicated in children • can cause fatal myocardial failure, metabolic acidosis, hypoxia, rhabdo
His seizure resolves after 3 doses of Ativan, and 2 doses of Fosphenytoin. After two hours he is still “post-ictal”. What should you think about?
STATUS EPILEPTICUS -- TYPES • Generalized non-convulsive convulsive • Partial • Psychogenic
NON-CONVULSIVE GENERALIZED STATUS • “Spike-wave stupor” • mental dullness, confusion, clumsiness • slow or monosyllabic speech • EEG diagnosis • diazepam universally effective
PSYCHOGENIC STATUS • 25-50% also have epileptic seizures • differentiating from status non-noxious stimuli noxious stimuli presentation EEG
Why is there a sense of urgency when treating status epilepticus?
STATUS EPILEPTICUS -- SEQUELAE • 3 factors 1) damage by acute insult 2) systemic stress from motor convulsions - exhaustion of metabolic supply 3) injury from repetitive electrical discharges in CNS and glutamate release
STATUS EPILEPTICUS -- SYSTEMIC STRESS • Cardiovascular--rate, rhythm, BP • Respiratory--insufficiency, pulmonary edema • Biochemical • acidosis, BUN, potassium • glucose, sodium, hypoxemia • Autonomic -- fever, secretions • Renal -- rhabdomyolosis, ARF Shorvon2001
STATUS EPILEPTICUS -- MORBIDITY & MORTALITY • 3-15% mortality • 5-40% residual neurologic deficit • most closely related to etiology of status • Maytal study (children): Idiopathic, noncompliance, & febrile status had NO M&M