Download
1 / 42
430 likes | 461 Views
Cardiac arrhythmias: commonly occur in the presence of preexisting heart disease the most common cause of death in patients with a myocardial infarction the most serious manifestation of digitalis toxicity, anesthesia, hyperthyroidism, and electrolyte disorders. Antiarrhythmic Drugs.

E N D
Cardiac arrhythmias: commonly occur in the presence of preexisting heart disease the most common cause of death in patients with a myocardial infarction the most serious manifestation of digitalis toxicity, anesthesia, hyperthyroidism, and electrolyte disorders. Antiarrhythmic Drugs
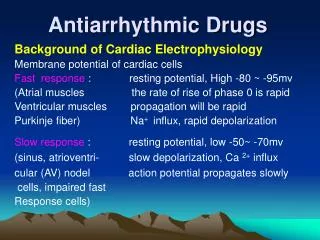
Pathophysiology What Is an Arrhythmia? Normal electrical cardiac function (normal sinus rhythm, NSR) is dependent on generation of an impulse in the normal sinoatrial (SA) node pacemaker and its conduction through the atrial muscle, through the atrioventricular (AV) node, through the Purkinje conduction system, to the ventricular muscle. Antiarrhythmic Drugs
Criteria of normal cardiac rhythm: 1-heart rate between 60-100 beat per min. 2-beat should be originate from SA node. 3-beat should pass through normal conductive pathway. 4- beat should be conducted with normal velocity. So : Normal cardiac rhythm should have: 1-normal impulse generation 2-normal impulse conduction.
Pathophysiology What Is an Arrhythmia? Normal pacemaking and conduction require normal action potentials (dependent on sodium, calcium, and potassium channel activity) under appropriate autonomic control. Arrhythmias (also called dysrhythmias) are any rhythm that is not normal sinus rhythm is an arrhythmia. Antiarrhythmic Drugs
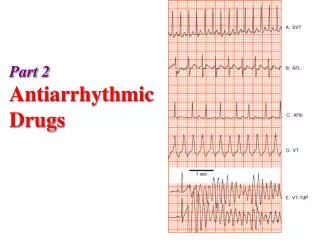
Arrhythmogenic Mechanisms Abnormal automaticity and abnormal (reentrant) conduction are the 2 major mechanisms for arrhythmias. A few of the clinically important arrhythmias are atrial flutter, atrial fibrillation (AF), atrioventricular nodal reentry (a common type of supraventricular tachycardia[SVT]), premature ventricular beats (PVBs), ventricular tachycardia (VT), and ventricular fibrillation (VF). Antiarrhythmic Drugs
Torsade de pointes is a ventricular arrhythmia of great pharmacologic importance because it is often induced by antiarrhythmic and other drugs that change the shape of the action potential and prolong the QT interval. Torsades is also associated with long QT syndrome, a heritable abnormal prolongation of the QT interval caused by mutations in the IK or INa channel proteins. Antiarrhythmic Drugs
Normal Electrical Activity in the Cardiac Cell The cellular action potentials are the result of ion fluxes through voltage-gated channels and carrier mechanisms. In most parts of the heart, sodium current (INa) dominates the upstroke (phase 0) of the action potential (AP) and is the most important determinant of its conduction velocity. After a very brief activation, the sodium currententers a more prolonged period of inactivation, Antiarrhythmic Drugs
Normal Electrical Activity in the Cardiac Cell In the calcium-dependent AV node, calcium current (ICa) dominates the upstroke and the AP conduction velocity (phase 1). The plateau of the AP (phase 2) is dominated by calcium current (ICa) and one or more potassium-repolarizing currents (referred to as a class as IK). At the end of the plateau, IK causes rapid repolarization (phase 3). Antiarrhythmic Drugs
Normal Electrical Activity in the Cardiac Cell The refractory period of most cardiac cells (the sodium-dependent cells) is a function of how rapidly sodium channels recover from inactivation. Recovery from inactivation depends on: 1-membrane potential, which varies with repolarization time and the extracellular potassium concentration. 2- on the actions of drugs that bind to the sodium channel (ie, sodium channel blockers). Antiarrhythmic Drugs
Antiarrhythmic drugs act on 1 or more of the 3 major currents (INa, ICa, IK) or on the β-adrenoceptors that modulate these currents. Similarly, in the calcium-dependent AV node, the duration of refractoriness is dependent on the rate of recovery from inactivation of the calcium channels. Antiarrhythmic Drugs
Drug Classification 1. Sodium channel blockers 2. Beta-adrenoceptor blockers 3. Potassium channel blockers 4. Calcium channel blockers The miscellaneous group includes adenosine, potassium ion, and magnesium ion. Antiarrhythmic Drugs
Group 1 Antiarrhythmics (Local Anesthetics) Prototypes The group 1 drugs are further subdivided on the basis of their effects on AP duration. Group 1A agents (prototype procainamide ) prolong the AP. Group 1B drugs (prototype lidocaine ) shorten the AP in some cardiac tissues. Group 1C drugs (prototype flecainide ) have no effect on AP duration. Antiarrhythmic Drugs
Mechanism of Action slow or block conduction in ischemic and depolarized cells and slow or abolish abnormal pacemakers wherever these processes depend on sodium channels. The most selective agents (those in group 1B) have significant effects on sodium channels in ischemic tissue, but negligible effects on channels in normal cells. In contrast, less selective group 1 drugs (groups 1A and 1C) cause some reduction of INa even in normal cells. Group 1 Antiarrhythmics(Local Anesthetics)
Drugs with Group 1A Actions Procainamide 1A prototype. (quinidine & disopyramide). Amiodarone(group 3), has typical group 1A actions. • These drugs affect both atrial and ventricular arrhythmias. • They block INa, and therefore slow conduction velocity in the atria, Purkinje fibers, and ventricular cells. • At high doses they also slow AV conduction.→ ↓ventricular conduction results in ↑QRS duration in the ECG. • In addition, the 1A drugs block IK and slow repolarization. Group 1 Antiarrhythmics(Local Anesthetics)
Drugs with Group 1B Actions Lidocaine prototype 1B drug used IV or IM routes. Mexiletineorally active 1B agent. BOTH drugs selectively affect ischemic or depolarized Purkinje and ventricular tissue and have little effect on atrial tissue. Phenytoin (anticonvulsant) is sometimes classified with the group 1B antiarrhythmic agents because it can be used to reverse digitalis-induced arrhythmias. Group 1 Antiarrhythmics(Local Anesthetics)
Drugs with Group 1C Actions Flecainide prototype drug with group 1C actions. • It has no effect on ventricular AP duration or the QT interval. • It is powerful depressant of INa, and can markedly slow conduction velocity in atrial and ventricular cells. • It increases the QRS duration of the ECG. Group 1 Antiarrhythmics(Local Anesthetics)
Clinical Uses of Group 1A Drugs: Procainamideused in all types of arrhythmias: atrial and ventricular arrhythmias are most responsive. Quinidine and disopyramide have similar effects but are used much less frequently. Procainamide is also commonly used in arrhythmias during the acute phase of myocardial infarction. Group 1 Antiarrhythmics(Local Anesthetics)
Toxicities of Group 1A Drugs: Procainamide may cause hypotension (parenterally) and a reversible syndrome similar to lupus erythematosus. Quinidine causes cinchonism (headache, vertigo, tinnitus); cardiac depression; GIT upset; and autoimmune reactions (eg, thrombocytopenic purpura). Quinidinereduces digoxin clearance and may increase the serum concentration of the glycoside significantly. Group 1 Antiarrhythmics(Local Anesthetics)
Toxicities of Group 1A Drugs: • Disopyramide has marked antimuscarinic effects and may precipitate heart failure. All group 1A drugs may precipitate new arrhythmias. • Hyperkalemia usually exacerbates the cardiac toxicity of group 1 drugs. • Treatment of overdose with these agents : sodium lactate (to reverse drug-induced arrhythmias) and pressorsympathomimetics(to reverse drug-induced hypotension). Group 1 Antiarrhythmics(Local Anesthetics)
Clinical Uses of Group 1B Drugs: • Lidocaine is useful in acute ischemic ventricular arrhythmias, after MI. Atrial arrhythmias are NOT responsive unless caused by digitalis. • Mexiletine has similar actions and is given orally. • Lidocaine is given I.V or I.M. It is never given orally because it has a very high first-pass effect and its metabolites are potentially cardiotoxic. Group 1 Antiarrhythmics(Local Anesthetics)
Toxicities of Group 1B Drugs: Lidocaine and mexiletine cause local anesthetic toxicity (ie, [CNS] stimulation, including convulsions); cardiovascular depression (usually minor); and allergy (rashes but may extend to anaphylaxis). These drugs may also precipitate arrhythmias, but this is much less common than with group 1A drugs. Hyperkalemia increases cardiac toxicity. Group 1 Antiarrhythmics(Local Anesthetics)
Group 1C Drugs Flecainide is effective in both atrial and ventricular arrhythmias. Flecainide and its congeners are more likely than other antiarrhythmic drugs to exacerbate or precipitate arrhythmias (proarrhythmic effect).. For this reason, the group 1C drugs are now restricted to use in persistent arrhythmias that fail to respond to other drugs. Group 1C drugs also cause local anesthetic-like CNS toxicity. Hyperkalemia increases the cardiac toxicity of these agents. Group 1 Antiarrhythmics(Local Anesthetics)
Prototypes, Mechanisms, and Effects Propranolol and esmolol (prototypic antiarrhythmicβ-blockers) mechanism in arrhythmias is cardiac β-adrenoceptor blockade and reduction in cAMP, which results in the reduction of both INa and ICa & suppression of abnormal pacemakers. These drugs have direct local anesthetic (sodium channel-blocking) effect in the heart, but this is rare at the concentrations achieved clinically. Sotalol and amiodarone, generally classified as group 3 drugs, also have group 2 β-blocking effects. Group 2 Antiarrhythmics (Beta Blockers)
Clinical Uses & Toxicities: Esmolol a very short-acting β-blocker for I.V administration, used exclusively in acute arrhythmias. Propranolol,metoprolol, and timolol are commonly used as prophylactic drugs in patients who have had a myocardial infarction. provide a protective effect for 2 yrs or longer after the infarct. patients with arrhythmias are often more prone to β-blocker-induced depression of cardiac output than are patients with normal hearts. Group 2 Antiarrhythmics (Beta Blockers)
Prototypes Dofetilide and ibutilide are typical group 3 drugs. Sotalol is a chiral compound (ie, it has 2 optical isomers). One isomer is an effective β-blocker, and both isomers contribute to the antiarrhythmic action. The clinical preparation contains both isomers. Amiodarone it blocks the same K channels and markedly prolongs AP duration as well as blocking sodium channels. Dronedarone is a new drug, similar to amiodarone but less efficacious and less toxic. Group 3 Antiarrhythmics(Potassium IK Channel Blockers)
Mechanism and Effects They produce AP prolongation by blockade of IK potassium channels that are responsible for the repolarization of the AP. Sotalol, ibutilide, dofetilide, and amiodarone (and group 1A drugs) produce this effect on most cardiac cells; the action of these drugs is, therefore, apparent in the ECG as an increase in QT interval. Group 3 Antiarrhythmics(Potassium IK Channel Blockers)
Clinical Uses and Toxicities Sotalol is available by the oral route. It may precipitate torsade de pointes arrhythmia as well as signs of β-blockade such as sinus bradycardia and asthma. Ibutilide and dofetilide are recommended for atrial flutter and fibrillation. Their most important toxicity is induction of torsade de pointes. Group 3 Antiarrhythmics(Potassium IK Channel Blockers)
Amiodarone: A Special Case Amiodarone is useful in most types of arrhythmias and is considered the most efficacious of all antiarrhythmic drugs. This may be because it has a broad spectrum: It blocks sodium, calcium, and potassium channels and β-adrenoceptors. Because of its toxicities, amiodarone is approved for use mainly in arrhythmias that are resistant to other drugs. Group 3 Antiarrhythmics(Potassium IK Channel Blockers)
Amiodarone: A Special Case Amiodarone causes microcrystalline deposits in the cornea and skin, thyroid dysfunction (hyper- or hypothyroidism), paresthesias, tremor, and pulmonary fibrosis,&rarely causes arrhythmias. Dronedarone , an amiodarone analog. Like amiodarone, it acts on sodium, potassium, and calcium channels but at present it is approved only for the treatment of atrial fibrillation or flutter. Group 3 Antiarrhythmics(Potassium IK Channel Blockers)
Prototype Verapamil is the prototype. Diltiazem is also an effective antiarrhythmic drug. Nifedipine and the other dihydropyridines are not useful as antiarrhythmics, probably because they decrease arterial pressure enough to evoke a compensatory sympathetic discharge to the heart. The latter effect facilitates rather than suppresses arrhythmias. Group 4 Antiarrhythmics(Calcium Channel Blockers)
Mechanism and Effects Verapamil and diltiazem are effective in arrhythmias that must cross calcium-dependent cardiac tissue (eg, the AV node). These agents cause selective depression of calcium current. AV conduction velocity is decreased and effective refractory period increased by these drugs. PR interval is consistently increased. Group 4 Antiarrhythmics(Calcium Channel Blockers)
Clinical Use and Toxicities Effective for converting AV nodal reentry (nodal tachycardia) to normal sinus rhythm. Their major use is in the prevention of these nodal arrhythmias. These drugs are orally active; and also parenteralIy. Toxicity of these drugs is excessive pharmacologic effect, because cardiac contractility, AV conduction, and blood pressure can be significantly depressed. These agents should be avoided in ventricular tachycardias. Amiodarone has moderate calcium channel-blocking activity. Group 4 Antiarrhythmics(Calcium Channel Blockers)
Adenosine It is a normal component of the body, if given I.V in high doses (6–12 mg), it slows or completely blocks conduction in the AV node, probably by hyperpolarizing this tissue (through increased IK1) and by reducing calcium current. Adenosine is extremely effective in abolishing AV nodal arrhythmias, and because of its very low toxicity it has become the drug of choice for this arrhythmia. Miscellaneous Antiarrhythmic Drugs
Adenosine has an extremely short duration of action (about 15 s). Toxicity includes flushing and hypotension, but because of their short duration these effects do not limit the use of the drug. Transient chest pain and dyspnea (probably due to bronchoconstriction) may also occur. Miscellaneous Antiarrhythmic Drugs
Potassium Ion Potassium depresses ectopic pacemakers, including those caused by digitalis toxicity. Hypokalemia is associated with an increased incidence of arrhythmias, especially in patients receiving digitalis. Conversely, excessive potassium levels depress conduction and can cause reentry arrhythmias. Therefore, when treating arrhythmias, serum potassium should be measured and normalized if abnormal. Miscellaneous Antiarrhythmic Drugs
Magnesium Ion Magnesium appears to have similar depressant effects as potassium on digitalis-induced arrhythmias. Magnesium also appears to be effective in some cases of torsade de pointes arrhythmia. Miscellaneous Antiarrhythmic Drugs