Download
1 / 57
590 likes | 1.01k Views
:- BLOOD GAS ANALYSIS :- Dr. T.C. Kriplani Professor & Head Department of Anaesthesiology NSCB Medical College & Hospital, JABALPUR (M.P.). POLIO – EPIDEMIC 1952- COPENHAGEN (DENMARK). DR. BJORN IBSEN. Q. What is the difference between : Blood gas analysis & Blood gas monitoring.

E N D
:- BLOOD GAS ANALYSIS :- Dr. T.C. Kriplani Professor & Head Department of Anaesthesiology NSCB Medical College & Hospital, JABALPUR (M.P.)
Q. What is the difference between : • Blood gas analysis • & • Blood gas monitoring Ans : Blood gas monitor is a patient dedicated device that measures arterial pH, PaCO2 and PaO2 without permanently removing blood. For blood gas analysis – Blood is removed from patient
Q. What are the principles of Gas analysis ? • Ans : • Chemical (Haldane, Orsat-Henderson & Van Slyke) • Physical (Magnetic, infrared, gas chromatography) • Specific electrodes
Q. What is the difference between electrode & optode ? • Ans : • Electrode : Sensor that operates via electrochemical • properties • Optode : Sensor that operates via optical detection • of altered light
Q. Who developed O2 electrode Ans : Dr. Leland Clark in 1956
Q. Who developed CO2 electrode Ans : Dr. John Severinghaus in 1959
Q. What are the sites from where blood can be drawn for blood gas analysis ? • Ans : • Usually from peripheral art. (Radial, Brachial, Femoral or Dorsalis pedis) • Arterialised capillary sample • Rare cases venous blood is used
Q. What are indications & contraindications of arterial blood gas analysis ? • Ans : • Indications: • To evaluate the adequacy of ventilation • To Quantitate patient’s response to therapeutic intervention • To monitor severity & progression of documented disease process • Contraindications: • -ve result of Allen’s test • Coagulopathy or medium to high dose anticoagulation therapy (Heparin, Coumadin, streptokinase, Caprostat) • Femoral puncture avoided outside hospital • Arterial puncture not performed distal to surgical shunt
Q. What are the complications of Arterial Puncture? • Ans : • Arteriospasm, Haematoma, Emboli (Air or clotted blood), Anaphylaxis if LA is used, Haemorrhage, Trauma to vessel, Arterial occlusion, Vasovagal response and Pain
Q. How Allen’s test is performed ? What precautions should be taken while taking the sample ? • Ans : Allen E.V. (1929) • Pt. closes hand as tightly as possible for 1 minute in order to squeeze out blood • Compress radial art. at wrist • Open the hand (extend fingers) • Note the return of colour • Full blushing – 7 seconds • Borderline – 8 – 14 seconds • Abnormal (-ve test) - > 14 seconds • LA – prevents arterial spasm, softens skin, increases subcutaneous space (working room), • Ringe syringe with Heparin 1 in 1000
Q. How arterialised capillary sample is taken ? • Ans : • Site – Finger, toe, heel or ear lobe • Wrapping in warm pad (40-430 C) for 10 minutes • Or • Massage ear lobe for 2-3 minutes • Heparinised capillary tube should be sealed after • collecting sample with clay at one end • Short steel wire is inserted then other end is sealed • Steel wire is moved with magnet to mix the sample
Q. How to take an arterial blood gas sample ? • Ans : • Syringe with 22 to 23 G needle for radial artery • puncture • Bevel facing up 20-300 angle, wrist extended 20- • 300 • 0.25 mL Heparin 1000 IU/mL concentration do • coating and discard rest • Send for analysis within 5-10 minutes or else store • in Ice child water (40C) maximum upto 60 minutes
Q. What is the difference between : • Acidosis & Acidaemia • or • Alkalosis & Alkalaemia Ans : In acidosis and alkalosis – Acid base disturbance is at cellular level, there is a change in PaCO2 or in HCO3- but there is no change in pH Where as in acidaemia there is change in pH below normal (< 7.36) similarly in alkalaemia pH goes above normal (> 7.44)
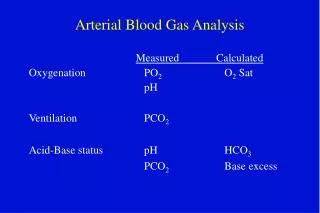
Q. What values are returned from ABGs ? Ans : 3-5 values are actually measured (pH, PaO2, PaCO2, Hb & O2 saturation) all remaining values are calculated like ABC, TCO2, SBC, BE, SBE
Q. What is the actual bicarbonate and what is standard bicarbonate ? • Ans : • Actual bicarbonate (ABC) is calculated from measured pH and PCO2 of whole blood sample • Standard bicarbonate (SBC) is simply a measure of bicarbonate concentration under standard conditions i.e., bicarbonate concentration in plasma of fully oxygenated blood which has been equilibrated to a PaCO2 of 40 mm of Hg at 370 C
Q. What are primary and secondary acid base derangements ? Ans : Primary is the cause of acid-base drangement where is the secondary is the compensatory change. The end point is constant if compensation is in range. PaCO2/ HCO3- is constant.
Q. What are the changes in actual HCO3- in levels in acute and chronic respiratory acidosis ? • Ans : • Acute respiratory acidosis : 1 mm of Hg rise in PaCO2 = 0.1 mmol/L rise in actual HCO3- • Chronic respiratory acidosis : 1 mm of Hg rise in PaCO2 = 0.4 mmol/L rise in HCO3-
Q. What are the changes in actual HCO3- levels in acute and chronic respiratory alkalosis ? • Ans : • Acute : 1 mm of Hg fall in PaCO2 = 0.2 mmol/L fall in HCO3- • Chronic 1 mm of Hg fall in PaCO2= 0.5 mmol/L fall in HCO3-
Q. What are the changes in PaCO2 in metabolic acidosis and alkalosis ? • Ans : • Metabolic acidosis : 1 mmol/L fall in HCO3- = 1-1.3 mm of Hg fall in PaCO2 • Metabolic alkalosis : 1 mmol/L rise in HCO3- = 0.6 mm of Hg rise in PaCO2
Q. The rules of acid base interpretation are based on which variables ? • Ans : • On three variables pH, PCO2 & HCO3- • If outside normal range, it is abnormal • Normal range : • pH 7.36 to 7.44 • PaCO2 36 to 44 mm of Hg • HCO3- 22 to 26 mEq/L
Q. How a primary metabolic disorder is diagnosed ? • Ans : • If pH is abnormal • & • If pH and PaCO2 change in the same direction • (Known as RULE 1) • Metabolic acidosis – If pH & PCO2 are less than normal • Metabolic alkalosis – If pH & PCO2 are more than normal
Q. With a primary metabolic acid-base disorder if a superimposed respiratory acid-base disorder is present, How it is diagnosed ? • Ans : • If a change in PaCO2 is not to the expected change (normal, higher or lower than expected) a combined metabolic and respiratory acid-base disorder is diagnosed • (RULE 2)
Q. How a primary respiratory acid base disorder is diagnosed ? • Ans : • If pH and PaCO2 change in opposite direction • (RULE 3) • Respiratory acidosis pH PaCO2 • Respiratory alkalosis pH PaCO2
Q. How to differentiate acute and chronic respiratory acid-base disorder ? • Ans : • pH 0.008 x (PaCO2 – 40) = Acute respiratory • pH 0.003 to 0.008 x (PaCO2 – 40) = Chronic • respiratory • pH > 0.0008 x (PaCO2 – 40) mixed disorder • (RULE 4)
Q. How a mixed disorder (acidosis and alkalosis) is diagnosed ? • Ans : • If PaCO2 is abnormal and pH is unchanged • Example : PaCO2 50 mm of Hg & pH 7.46 • (RULE 5)
RULE ORIENTED ACID-BASE INTERPRETATION : Q. pH < 7.36 PCO2 – low – expected change or normal – unexpected change • Ans : • PCO2 – expected change (Diag. Primary metabolic acidaemia (RULE 1) • PCO2 unexpected change or normal (Diag. Primary metabolic acidaemia with superimposed respiratory disorder (RULE 2)
Q. pH < 7.36 PaCO2 is high (opposite change) • Ans : • Diag. Respiratory acidaemia (RULE 3)
Q. pH > 7.44 PaCO2 – high expected - unexpected • Ans : • PaCO2 high expected • Diag. Metabolic Alkalemia (RULE 1) • PaCO2 unexpected high or normal • Diag. Metabolic Alkalemia with respiratory disorder (RULE 2)
Q. pH > 7.44 PaCO2 – Low (acute or chronic) • Ans : • Diag. Primary Respiratory Alkalemia (RULE 3) • See pH change • Acute pH = 0.008 x (40-PaCO2) • Chronic pH = 0.003 - 0.008 x (40-PaCO2) • If the change is not according to calculation, then metabolic disorder is superimposed (RULE 4)
If pH is normal, but • PaCO2 is high • or • PaCO2 is low • Ans : • If PaCO2 is high (mixed disorder) respiratory acidosis + metabolic alkalosis • If PaCO2 is low (mixed disorder) respiratory alkalosis + metabolic acidosis • (RULE 5)
A 19 years old boy brought in emergency with history of injecting some drug. O/E respiration shallow 8/mt, responded to painful stimuli. • Arterial blood gases shows: • pH 7.2 • PaCO2 72 mm of Hg • ABC 26.5 mmol/L • SBC 26.0 mmol/L • BE 1.4 mmol/L • Ans : • Acute Respiratory Acidaemia
A 67 years old male with H/O cough and respiratory distress and chronic smoking came in emergency : • Arterial blood gases shows: • pH 7.36 • PaCO2 60 mm of Hg • ABC 32 mmol/L • SBC 30.0 mmol/L • BE +4 mmol/L • Ans : • Chronic respiratory acidosis (compensated) with metabolic alkalosis
A 18 years old girl was admitted in the hospital after an argument with her boy friend. She denied taking any medication. On examination chest clear, respiratory rate 34 / mt. Blood gas estimation shows : • pH 7.5 • PaCO2 26 mm of Hg • ABC 20 mmol/L • SBC 23.0 mmol/L • BE -1 mmol/L • Ans : • Acute Respiratory Alkalosis with less metabolic compensation
A 52 years old man brought in emergency with history of cough and pleuritic chest pain for few days increasingly becoming breathless: • Arterial blood gases shows: • pH 7.52 • PaCO2 13.6 mm of Hg • ABC 12.2 mmol/L • SBC 14.0 mmol/L • BE -8.2 mmol/L • Ans : • Chronic Respiratory Alkalemia with poor metabolic compensation
A 27 years old epileptic man had grand mal seizures. Convulsions stopped without any medication after 2 minutes. He was brought to casualty: • Arterial blood gases shows: • pH 7.26 • PaCO2 26 mm of Hg • ABC 12.2 mmol/L • SBC 12.9 mmol/L • BE -13.3 mmol/L • Ans : • Acute Metabolic Acidaemia with respiratory compensation
A 66 years old woman had cardiac arrest in casualty. Basic and advanced life support was started in casualty. While patient was being ventilated blood sample was taken: • Arterial blood gases shows: • pH 6.86 • PaCO2 38.9 mm of Hg • ABC 6.6 mmol/L • SBC 6.6 mmol/L • BE - 23.9 mmol/L • Ans : • Acute Metabolic Acidaemia
A 33 years old man with insulin dependent diabetes brought to emergency department not well for 3 days c/o frequency of urination, fever, nausea, sweating had not been eating hence not taking insulin: • Arterial blood gases shows: • pH 7.2 • PaCO2 22 mm of Hg • ABC 5.4 mmol/L • SBC 7.5 mmol/L • BE -26 mmol/L • Ans : • Metabolic Acidaemia with poor compensation
A 68 years old man c/o severe chest pain and shortness of breath. O/E cold and clammy R/R 8 mt brought in emergency: • Arterial blood gases shows: • pH 6.99 • PaCO2 109.5 mm of Hg • ABC 15.5 mmol/L • SBC 15.3 mmol/L • BE -12.4 mmol/L • Ans : • Combined respiratory and metabolic Acidaemia
A 64 years old woman had persistent cough and gradual increase in breathlessness. H/o of smoking 30-40 cigarettes a day: • Arterial blood gases shows: • pH 7.38 • PaCO2 63.2 mm of Hg • ABC 37.0 mmol/L • SBC 33.4 mmol/L • BE +5.3 mmol/L • Ans : • Respiratory Acidosis
A 40 years old woman who had taken overdose of Dothiepin (a tricyclic antidepressant) 2 hrs previously. She was unconscious with a shallow breathing RR 8 / mt. • Arterial blood gases shows: • pH 6.76 • PaCO2 46.5 mm of Hg • ABC 6.5 mmol/L • SBC 6.2 mmol/L • BE -29 mmol/L • Ans : • Mixed Respiratory and Metabolic Acidaemia
A patient admitted in surgical ward was on gastric aspiration through Ryle’s tube because of persistent vomitings: • Arterial blood gases shows: • pH 7.5 • PaCO2 50 mm of Hg • ABC 35 mmol/L • SBC 32 mmol/L • BE +8 mmol/L • Ans : • Acute Metabolic Alkalaemia
A 26 years old man having vomiting and diarrhoea from 4 days came in emergency: • Arterial blood gases shows: • pH 7.48 • PaCO2 43 mm of Hg • ABC 31 mmol/L • SBC 30 mmol/L • BE +4.5 mmol/L • Ans : • Metabolic Alkalaemia
A 51 years old woman presented in emergency department c/o of shortness of breath. The symptoms were present from years. She had no other medical problems: • Arterial blood gases shows: • pH 7.48 • PaCO2 17.9 mm of Hg • ABC 12.5 mmol/L • SBC 14.5 mmol/L • BE -6.6 mmol/L • Ans : • Chronic Respiratory Alkalaemia
A 69 years old woman after cholecystectomy had paralytic ileus. She had regular gastric aspiration from last 10 days: • Arterial blood gases shows: • pH 5.8 • PaCO2 53.1 mm of Hg • ABC 49 mmol/L • SBC 46 mmol/L • BE +20 mmol/L • Ans : • Metabolic Alkalaemia
A 30 years old lady attempted to commit suicide by throwing herself into a canal having taken overdose of alcohol . Passing policeman saved her & brought her to casualty. O/E she was pale, cold and confused. Her tympanic temperature was 28.40C, R/R 18/mt, PR 108/mt, BP 136/90 chest – bilateral crepts and ronchi. • Arterial blood gases on breathing room air shows: • pH 7.23 • PaCO2 41.5 mm of Hg • ABC 16.7 mmol/L • SBC 16.4 mmol/L • BE -10.2 mmol/L • PaO2 86.0 mm of Hg • Ans : • Combined metabolic and respiratory acidaemia
What is anion gap ? • Ans : • Anion gap is an acid-base parameter that is used to evaluate patients with metabolic acidosis to determine whether metabolic acidosis is due to accumulation of acids (lactic or ketoacids) or loss of bicarbonate
How AG is estimated ? • Ans : • AG = Na+ - (Cl- + HCO3-) • = 10-12 mEq/L