Download

1 / 31
310 likes | 321 Views
Explore the fundamental principles of acid-base chemistry and how it relates to biochemical changes in the extracellular environment, including the role of strong ions, weak acids, and carbon dioxide. Learn about the Arrhenius and Brønsted-Lowry theories, as well as the Stewart approach to acid-base balance.

E N D
Acid-base abnormalities should be seen as resulting from other biochemical changes in the extracellular environment strong ions (Na+ , Cl- , K+ , SO4 2- , Mg2+ , Ca2+) weak acids(albumin , phosphate) carbon dioxide To maintain electrical neutrality OH- H+
PHYSICAL CHEMISTRY OF WATER H2O + H+ OH- fundamental to the existence of life H H O O H O 105o H H H
PHYSICAL CHEMISTRY OF WATER 1.0 × 10−7 mmol/L H2O + H+ OH- 25o C Keq H2 O = [H+ ][OH− ]Keq H2 O = Keq (55.5) = Kw = [H+ ][OH− ] A solution is considered acidic if :([H+ ] > 1.0 × 10−7 mmol/L, [OH− ] < 1.0 × 10−7 mmol/L). A solution is considered alkaline if ([H+ ] < 1.0 × 10−7 mmol/L, [OH− ] > 1.0 × 10−7 mmol/L).
ACIDSANDBASES • Svante Arrhenius in 1903 established the foundations of acid-base chemistry. • In an aqueous solution, an Arrhenius acid is any substance that delivers a hydrogen ion into the solution. (HCl)A base is any substance that delivers a hydroxyl ion into the solution. (KOH) • In 1909, L.J. Henderson coined the term acid-base balance. • Hasselbalch (1916)H2O + CO2 → H2CO3 →[H+] + [HCO3-] • pH = pKa + log [HCO3− ] / [H2 CO3 ] • pH = 6.1 + log [HCO3− ] / PCO2 × 0.03
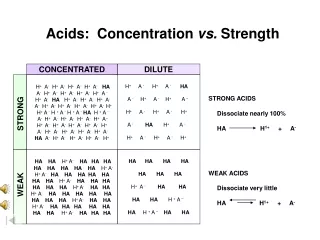
The degree of dissociation of substances in water determines whether they are strong acids or strong bases. • Lactic acid, pKa of 3.4, is a strong acid. • Carbonic acid, pKa of 6.4, is a weak acid. • Similarly, ions such as sodium, potassium, and chloride, which do not easily bind other molecules, are consideredstrong ions; they exist free in solution. • Strong cations (Na+ , K+ , Ca2+ , Mg2+ ) act as Arrhenius bases • Strong anions (Cl- , LA- [lactate], ketones, sulfate, formate) act as Arrhenius acids. • One problem with the Arrhenius theory:ammonia (NH3 ), sodium carbonate (Na2 CO3 ), and sodium bicarbonate (NaHCO3) • In 1923, Brønsted and Lowry They defined acids as proton donors and bases as proton acceptors.
NH3 + H2 O ⇌ NH4 + + OH−In this situation, water is the proton donor, the Brønsted-Lowry acid, and ammonia the proteon acceptor, the Brønsted-Lowry base. • HCl + H2 O → H3 O+ + Cl−In the previous reaction, hydrogen chloride acts as a Brønsted-Lowry acid and water as a Brønsted-Lowry base. • CO2 + H2 O ⇌ H2 CO3 ⇌ H+ + HCO3− In this reaction, carbon dioxide is hydrated to carbonic acid, a Brønsted-Lowry acid, which subsequently dissociates to hydrogen (H+ ) and bicarbonate (HCO3 - ) ions.
STEWART APPROACH TO ACID-BASE BALANCE • What Determines the Acidity or Alkalinity of a solution? • The molar concentration of hydrogen and hydroxide must be used to reflect the relative acidity and alkalinity of a solution. • The pH scale, developed by Sorenson in the 1920s. • Neutral pH for pure water is 7.0 (1.0 × 10−7 mmol/L). • Physiological pH for the ECF is 7.4, which is alkaline. • The pH of the intracellular space is 6.8 to 7.0
STEWART APPROACH TO ACID-BASE BALANCE • 1. Electrical neutrality. In aqueous solutions in any compartment, the sum of all of the positive charged ions must equal the sum of all of the negative charged ions. • 2. Dissociation equilibria. The dissociation equilibria of all incompletely dissociated substances, as derived from the law of mass action, must be satisified at all times. • 3. Mass conservation. The amount of a substance remains constant unless it is added, removed, generated, or destroyed. • The total concentration of an incompletely dissociated substance is the sum of concentrations of its dissociated and undissociated forms.
Strong Ions • The most abundant strong ions in the extracellular space are Na+ and Cl- . • Other important strong ions include K+, SO42- , Mg2+, and Ca2+. • If NaOH and HCl, added to solution([Na+ ] − [Cl− ])+([H+ ] − [OH− ])=0 • In this system, ([Na+− [Cl−]) must determine [H+] and [OH−].
In any solution, the sum total of the charges imparted by strong cations minus the charges from strong anions represents the SID. • The SID independently influences hydrogen ion concentration. • In human ECF, the SID is positive. • SID is an independent variable and [H+] and [OH-] are dependent, meaning that the addition of hydrogen ions alone (without strong corresponding anions) cannot influence the pH of the solution
Weak Acid Buffer Solutions • These are partially dissociated compounds whose degree of dissociation is determined by the prevailing temperature and pH. • The predominant molecules in this group are albumin and phosphate. • Stewart used the term ATOT to represent the total concentration of weak ions that influenced acid-base balance
Weak Acid Buffer Solutions • KA [HA] = KA [H+] [A−] • [HA] + [A− ] = [ATOT ] • [H+]× [OH−] = Kw (water dissociation) • [SID] + [H+] − [A−] − [OH−] = 0 (electrical neutrality) • SID and ATOT are independent variables • Kw and KA are constants • [HA], [H+], [OH-], and [A-] are dependent variables.
Carbon Dioxide • 1- carbon dioxide, denoted CO2 (d);2- carbonic acid (H2 CO3) 3- bicarbonate ions (HCO3- ) 4- carbonate ions (CO32- ) • [CO2 (d)] = [SCO2] × PCO2 • [CO2 (d)] × [OH− ] = K1 × [HCO3− ] • [H+ ] × [HCO3− ] = Kc × PCO2 • [H+ ] × [CO32− ] = K3 × [HCO3− ]
Factors Independently Influencing Water Dissociation • Water dissociation equilibrium: [H+ ] × [OH- ] = KW • Weak acid dissociation equilibrium: [H+ ] × [A- ] = KA× [HA] • Conservation of mass for weak acids: [HA] + [A- ] = [ATOT ] • Bicarbonate ion formation equilibrium:[H+ ] × [HCO3 - ] = KC× PCO2 • Carbonate ion formation equilibrium: [H+ ] × [CO3 2- ] = K3× [HCO3- ] • Electrical neutrality: [SID] + [H+ ] - [HCO3 - ] - [A- ] - [CO32- ] - [OH- ] = 0
[H+ ]4 + ([SID] + KA ) × [H+ ]3 + (KA × ([SID] − [ATOT ]) − Kw − Kc × PCO2 ) × [H+ ]2 − (KA × (Kw + Kc × PCO2 ) − K3 × Kc × PCO2 ) × [H+ ] − KA × K3 × Kc × PCO2 = 0 • [H+ ] is a function of SID, ATOT, PCO2 , and several constants. • All other variables, most notably [H+], [OH-], and [HCO3-], are dependent and cannot independently influence the acid-base balance
ACID-BASE ABNORMALITIES • Stewart approach: SID, ATOT, PCO2 Traditional approach • Alterations in (PaCO2) tension : respiratory acidosis or alkalosis • Alterations in blood chemistry : ( HCO3- , BE )metabolic acidosis, or alkalosis
ACID-BASE ABNORMALITIES Respiratory Acid-Base Abnormalities • Respiratory acidosis → acute rise in PaCO2principally because of respiratory failure • Clinically, : (signs of CO2 retention)Cyanosis, vasodilatation, and narcosis. • Respiratory alkalosis → acute decrease in PaCO2 (caused by hyperventilation.) • Clinically : Vasoconstriction: light-headedness, visual disturbances, dizziness, and perhaps hypocalcemia
Respiratory acidosis • Causes a rapid increase in [H+]. • Compensation for hypercarbia is slow • Increased urinary excretion of chloride • There is a concomitant increase in the serum bicarbonate, reflecting a higher total CO2 load, rather than compensation. • The acuity of respiratory failure can be deduced by looking at the relative ratio of CO2 to HCO3– • Many investigators have suggested that respiratory acidosis may not necessarily be harmful. • There has been extensive clinical experience with "permissive hypercapnia" for acute respiratory failure, which appears to be well tolerated.
ACID-BASE ABNORMALITIES Metabolic Acid-Base Disturbances • Metabolic acid-base abnormalities →SID or ATOT, or both • An increase in the SID causes alkalemia • A decrease in the SID causes acidemia (e.g., hyperchloremia, lacticemia, dilutional acidosis ) • Metabolic acidosis is of clinical significance for two reasons: • pathologies arising from the acidosis itself • pathologies arising from the cause of the acidosis(Increased ionized calcium → vasodilation, diminished muscular performance (particularly myocardial), and arrhythmias )
REGULATION OF ACID-BASE BALANCE • A buffer is a solution of two or more chemicals that minimizes changes in pH in response to the addition of an acid or base. • Most buffers are weak acids. Ideally, a buffer has a pKa that is equal to the pH, and an ideal body buffer has a pKa between 6.8 and 7.2. • The major source of acid in the body is CO2 , from which is produced 12,500 mEq of H+ each day. • The metabolic compensation for respiratory acidosis isincreasedSID by removal of chloride. • Volatile acid is principally buffered by hemoglobin. • Chloride shift:
Erythrocyte Buffering System And Chloride Shift
REGULATION OF ACID-BASE BALANCE • Metabolic acid is buffered principally by increased alveolar ventilation, producing respiratory alkalosis and extracellular weak acids. • These weak acids include :plasma proteins, phosphate, and bicarbonate. • The bicarbonate buffering system (92% of plasma buffering and 13% overall) is probably the most important extracellular buffer.
REGULATION OF ACID-BASE BALANCE • The major effect of the kidney on acid-base balance is related to renal handling of sodium and chloride ions. • In metabolic acidosis, chloride is preferentially excreted by the kidney. • In metabolic alkalosis, chloride is retained, and sodium and potassium are excreted. • In renal tubular acidosis, there is an inability to excrete Cl- in proportion to Na+ . • The diagnosis can be made by observing a hyperchloremic metabolic acidosis with inappropriately low levels of Cl- in the urine; the urinary SID is positive. • If the urinary SID is negative, the process is not renal. • Gastrointestinal losses (diarrhea, small bowel or pancreatic drainage), parenteral nutrition, excessive administration of saline; and the use of carbonic anhydrase inhibitors.