Download
1 / 21
210 likes | 358 Views
LEAST Lead Improving community response to lead poisoning in Galveston, in coordination with GISD July 9, 2008. Why is lead poisoning an issue in Galveston?. Background and current situation Plan. Lead exposure and cognition in children - Needleman.

E N D
LEAST Lead Improving community response to lead poisoning in Galveston, in coordination with GISD July 9, 2008
Why is lead poisoning an issue in Galveston? • Background and current situation • Plan
Lead exposure and cognition in children - Needleman • Groundbreaking study in 1979 showed negative correlation between tooth lead and cognitive development in “normal” children • Herbert Needleman, the lead investigator attacked for years by lead industry
Blood lead and IQ • Numerous studies confirmed effect of lead • Meta-analysis by Lanphear et al 2005 showed greatest effect at average BLL < 10 ug/dL, the CDC action level
Persistence of lead effect • Follow-up of original Needleman Cohort in adolescence showed that behavioral effects persist • Correlation between dentine lead and unfavorable education outcomes • Failure to graduate • Criminal behavior • Persistent hyperactivity
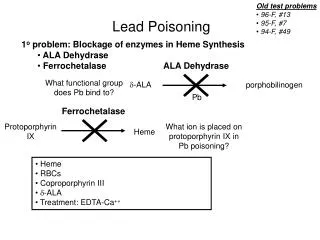
Mechanisms of toxicity in children • Lead interferes with brain development during rapid growth • Alters plasticity of synaptic formation and pruning • Complex interactions with neurotransmitter receptors and neurotransmitters • Some genetic polymorphisms identified but not well characterized yet
Childhood lead exposure in Galveston • Old housing stock and high proportion of disadvantaged families • Historical elevated blood lead rates about 20% (2% national average) • Loss of Federal funding after 2003 degraded program coordination • Report by Winnie Hamilton regenerated concern and resolve Hamilton et al., 2007
Where we are • Task Force created • Conflicting studies, concerns about data accuracy and applicability • Completeness of childhood sampling, and disparities • Uninsured or undocumented children • Problems with information systems vis a vis analysis and reporting • Multiple laboratories • Slow turnaround at DSHS • Coordination of reporting and case management • Concern about lead and special education • Need to raise funds for environmental interventions
Proposed Aims and Activities • Strengthen the evidence base • Reduce turnaround time for reporting of blood lead results • Improve coordination of information systems among agencies • Screen to catch “gap” kids • Lead and special education rates: links and appropriate responses • Public and provider education • Documentation to support fund-raising and environmental interventions • (Analysis of environmental samples)
1) Strengthen the evidence base on population exposure Why an additional study?
Baylor study flawed. • cited that Galveston children are 9 times more likely to be lead poisoned. • Data were incomplete. • Data presented covered 15 year period.
Need for precise measures of: • Accuracy and scope of screening through all UTMB clinics • Accurate and accessible blood lead measures • Charts will have to be independently reviewed for BLLs
Real data must drive decisions related to: • Additional screening needs • Interventions with at-risk populations • Educational enhancement (GISD) • Case management (UTMB/GCHD) • Pursuit of remediation $$ (City/County) • Disparities in testing and reporting (UTMB/GCHD/State Lab)
It is our moral imperative to do so. • We are not only in the community; in most cases, we are the community. • We bring skills to the table that no other single group can offer. • We must use our resources to ensure culturally and medically appropriate interventions at the grassroots level. • If we are part of the problem, we must be a part of the solution.
2) Reduce turnaround time for reporting Participate in DSHS pilot of on-line retrieval of results (Copia) Back-up plan: local analysis for Medicaid patients *Greatly reduces disparities, improves follow-up success 12 weeks 8-10 days
3) Improve information coordination among agencies • Linking GCHD with ClinLab and with Peds to develop reporting templates; plan to expand to other local providers • Copia coordinates demographic and other information automatically • Working on on-line information retrieval of DSHS results for GCHD * Provides more accurate reporting of screening coverage and results to CDC; improves follow up and reduces disparities
4) Screening for ages 0-5 • Catch “gap” kids through targeted screening events • Head Start physicals (0-2); health fairs; immunization drives; special events • On-site analysis and counseling (Lead Safe 2 Analyzer) • Immediate referral for exposed children *Enhance equity in identifying exposed children
5) Special education • Collaboration with GISD • Study design • Support development of appropriate health and education responses *Provides documentation of potential problem created for the educational system; provides guidance for further community planning
6) Public and provider education For the public • clinical encounters: 3-5 minute video, leaflets, improved counseling • public health events: on-site testing and counseling, leaflets, longer videos For providers • CCE’s • lectures *Public needs to be able to “self-protect” until funded environmental interventions are in place; providers must be brought on board whole-heartedly to ensure vigilant screening