Download
1 / 19
300 likes | 1.34k Views
Semen Analysis. Physiology of Seminal fluid . Semen is grey opalescent fluid which consists of suspension of spermatozoa in seminal plasma. It is made up of the secretions of all accessory glands of the male genital tract as well as testicular component . The Percentage Contribution of

E N D
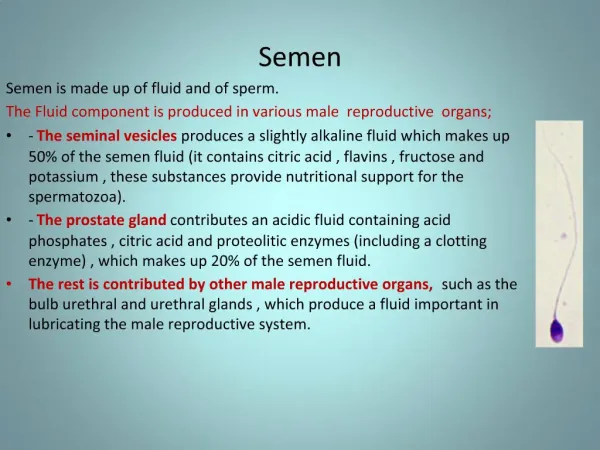
Physiology of Seminal fluid • Semen is grey opalescent fluid which consists of suspension of spermatozoa in seminal plasma. • It is made up of the secretions of all accessoryglands of the male genital tract as well as testicular component. The Percentage Contribution of Each of the Secretions in Seminal Fluid
Physiology of Seminal fluid • Prostatic Secretion • The prostatic fluid pH =6.5 • Enzymes: vesiculase • Spermine: bacteriostatic • Acid phosphatase • Citrates • Semonal Vesicle Secretion • Fructose: source of energy for sperms • especially needed for sperms motility • Prostaglandins: • Play a role in controlling sperm movement & • sperm penetration of cervical mucus • Fibrinogen-like substance : • Acted upon by enzyme vesiculase to • induce clotting that occurs in semen Two ejaculatory duct is formed by the union of the vas deferens with the duct of the seminal vesicle. They pass through the prostateand open into the urethra . During ejaculation, semen passes through the prostate gland, enters the urethra
Physiology of Seminal fluid • During ejaculation, each of the components that make up semen may be discharged from the urethra in a predetermined sequence First part: testicular component Second part: prostatic secretion Third part: vesicle secretion • Thus it is possible by careful collection of semen at least in part to separate out the secretions “split ejaculate”
Indication of Semen Analysis • Assessment of fertility / infertility (most common) • Determination of suitability of semen for artificial insemination • Follow up of fertility after cancer treatment by radio- or chemotherapy • Determination the effectiveness of vasectomy (Semen is repeatedly analyzed until azoospermia is detected) • Forensic purpose
SemenAnalysis Specimens: 2 samples should be collected for initial evaluation The interval between the two collections should not be less tha7 days or more than 3 weeks If the results of these assessments are markedly different, additional samples should be examined
Examination of Semen Macroscopic Examination • Volume • Liquefaction time • Appearance • pH • Viscosity Microscopic Examination • Sperm count • Sperm motility • Sperm viability • Sperm morphology • Agglutination • Antibodies coating of sperms Biochemical Tests • Fructose test • Acid phosphatase
Volume : (2-6ml/ ejaculation) Aspermia: total absence of ejaculation ( rare) Hypospermia or oligospermia: the seminal fluid is < 2ml Hyperspermia: volume > 10 ml Inflammatory process in seminal vesicle & to lesser extent in prostate ( spermia denotes seminal fluid not spermatozoa) Liquefaction time: Semen forms gel-like clot immediately after ejaculation Normally, semen sample liquefies within 15 -60 mint If prolongation must be recorded Appearance & Color: Normally, homogeneous grey opalescent appearance The color is due to high content of protein & presence of > 60 million sperms/ml Less opaque: if sperm concentration is very low White turbid: in inflammation and high WBCs Reddish: in haematospermia (RBCs in semen) Yellow: in patient with jaundice
Viscosity : A normal sample leaves small discrete drop when dropped In case of abnormal viscosity drop will form a thread more than 2 cm long High viscosity : can interfere determination of sperm motility pH : 7.2-8.0 in fresh semen pH more than 8.0 may be due to: • Acute disease of the seminal vesicles (increased secretion of seminal vesicles) • Delayed measurement (loss of CO2 ) Lowering of pH may be due: • Chronic inflammatory of seminal vesicles (nosecretion from seminal vesicles) • Contamination with urine (retrograde ejaculation) A pH < 7.0 with azoospermia Seminal fluid is composed of prostatic secretion only may be due to: • Obstruction of the ejaculatory ducts • Bilateral congenital absence of vasa difference
Sperm Count 20 million/ml (i.e. ~ 60 million / ejaculation) It is obtained by multiplying the sperm concentration by the volume Azoospermia: means no spermatocytes (male sterility) Oligozoospermia: < 20 million/ml (less than 50 million/ejaculation) Polyzoospermia: may reach 350 millions / ejaculation Decreased Sperm Count: • Vasectomy (should be 0 after 3-6 months) • Varicocele • Primary testicular failure • Secondary testicular failure • Congenital vas obstruction • Hyperprolactinemia
Assessment of Sperm Motility The motility of each spermatozoon is graded : • a = rapid progressive motility • b = slow or sluggish motility • c = non progressive motility • d = immotility Assessment of Sperm Viability • should be determined if the percentage of immotile spermatozoa exceeds 50 % • Supravital stain: • Eosin +/- Nigrosin • Viable do not take up the stain
Assessment of Sperm Morphology Normally the sperm count contains fewer than 20 % abnormal forms e.g. bitailed, short tailed , 2 heads …..etc.
Other cellular elements Leukocytes: • Normal < 1 x 106 /ml (or < 5/HPF) • If increased leukospermia or pyospermia may be associated with infection and poor sperm quality • When the number is increased, microbiological tests should be performed to investigate the presence of infection in any of the accessory glands Immature germ cells The round cells other than leukocytes, include round spermatids, spermatocytes, spermatogonia & exfoliative epithelial cells. Excessive shedding of immature germ cells usually results from impaired seminiferous tubule function as hypospermatogenises, varicocele & Sertoli cell dysfunction & associated with reduced in vitro fertilization
Agglutination Reported when motile sperm stick to each other in a definite pattern. Head-head Tail-tail Head-tail Immunological cause of infertility
Biochemical Tests Fructose Test: It is secreted for sperm nutrition from seminal vesicle. Impairment of seminal vesicular secretion will result in reduced fructose secretion in semen & the motility of the sperms will be reduced. Semen of men with ejaculatory duct obstruction or congenital absence of the seminal vesicles & vasa difference is characterized by: • Low fructose • Low volume • low pH • No coagulation • No characteristic semen odor Acid Phosphatase: This test is: • A marker of prostatic functions • Test for the presence of semen (In forensic Medicine)
Testing for Antibody coating of spermatozoa Sperms can induce immune response & produce antibodies. Sperm antibodies (IgA & IgG) may : • Cause agglutination of sperm • Cause reduction in motility • Inhibit the ability of sperm to penetrate cervical mucus • Impede binding of the sperm to the oocyte
Macroscopic Examination: Volume 2.0-6.0 ml ColorGrayish white Liquefaction: 15 - 60 minutes pH: 7.2 - 8.0 Microscopic Examination: Count>20 million/ml Motility > 50 % motile( grades a+b) or > 25% with progressive motility (grade a) within minutes Morphology > 30% normal form Viability> 75% viable WBC < 5 / HPF RBCNone Reference Ranges of Semen Analysis