Download
1 / 51
530 likes | 674 Views
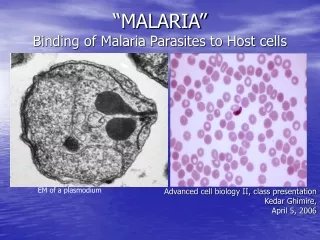
Introduction to Malaria. Remigius Okea, MD MPH Professor Emeritus American Hope Institute (AHI) Research Director: American Academy of Primary Care Research (AAPCR) Chairman Scientific Advisory Board of Tropical PharmMedics Research Institute First presented in 2003.

E N D
Introduction to Malaria Remigius Okea, MD MPH Professor Emeritus American Hope Institute (AHI) Research Director: American Academy of Primary Care Research (AAPCR) Chairman Scientific Advisory Board of Tropical PharmMedics Research Institute First presented in 2003
Review Objectives 1. Distribution • Understand malaria cycle • Transmission • Understand the treatment • Plasmodium life cycle (a basis for understanding the disease) • Pathophysiology • Brief description of health significance of Malaria • Symptoms and signs • Diagnosis • Differential diagnosis • Treatment (a)Modality (b)Drug classes and uses (c) Drug side effects
Significance • About 40% of the world’s population at risk • Worldwide clinical cases range from 300-500 million per year. • Worldwide 1.5-2.7 million deaths per year
Areas affected • Central and South America, • Hispaniola (Haiti and the Dominican Republic), • Africa, • Indian subcontinent, • Southeast Asia, • Middle East, • Oceania • Over 100 countries included
Plasmodium life cycle (see next slide for diagram) • Cycle A : Pre - Erythrocytic cycle • Cycle B : Erythrocytic cycle • Cycle C : Sporogonic cycle. This cycle occurs in the mosquito • The gamatocytic cycle is a development form the erythrocytic cycle. It is necessary to perpetuate the sporogonic cycle in the mosquito.
. .
Transmission • Causative agent: Plasmodium (falciparum, vivax, ovale and malariae) • Vehicle: Infected female Anopheles mosquitoes that bite between dusk to dawn during its primary feeding time. • Human to human transmission • Except for mosquitoes, no animal reservoirs for human malaria exists • Other modes of transmission: Congenital Blood transfusion (Induced Malaria)
Anopheles mosquito life cycle (Egg, Larva, Pupa and Adult)Adapted from CDC
Essential point to note for transmission to occur • Egg to adult stage takes 10 – 14 days (may be as short as 5 days) • Adult males live for 1 week • Adult females may live for 2 – 4 weeks • Females need blood meal to produce eggs. May take 2 – 3 days after that meal to complete egg production • Both males and females feed on sugar rich nectar • Once mosquito ingests plasmodium gametes, it takes 10 – 21 days (extrinsic incubation time) for the mosquito to be infective • Thus, mosquito must survive longer than the intrinsic incubation period for transmission to occur
Pathophysiology • Malaria parasite infect the RBC and utilize its energy source to multiply by binary fission • Lysis of RBC occur causing haemoglobinemia, anaemia and activation of the haematopoietic system leading to reticulocytosis. • Schizogony leads to release of pyrogen (necrotic factors and other cytokins) that resets the hypothalamic thermoregulatory center causing fever. • In the liver, malaria (especially severe P. falciparum) can cause acute hepatopathy with centrilobular necrosis, jaundice but no liver failure. • P Falciparum (occasionally others) may cause sequestration and cytoadherence of infected RBC to capillaries and post-capillary venules leading to cerebral edema or non-cardiac pulmonary edema (and other related symptoms).
Symptoms of uncomplicated malaria • Fever (to 41 C or higher), • Shaking chills, • Marked diaphoresis • Headache, • Dizziness, • Gastrointestinal symptoms, • Arthralgia, myalgia, back ache, • Dry cough • Fatigue • Loss of appetite
Signs of uncomplicated Malaria • Anemia, • Hyperpyrexia, • Splenomegally (after 4 days) • Hepathomegally (infrequent) • Hematuria • Abdominal tenderness • Hemodynamic instability • Mental status changes • Tarchypnoea
Complications • Haemolytic anaemia • Hyperthermia • Acute tubular necrosis and renal failure (may be associated with black water fever) • Cerebral oedema • Non-Cardiogenic pulmonary oedema • Acute hepatopathy (marked jaundice) • Hypoglycemia • Adrenal insufficiency-like syndrome • Cardiac dysrhythmia
Complications.. • Water and electrolyte imbalance • Lactic acidosis • Coexisting pneumonia • GIT syndromes (secretory diarrhoea, dysentery) Complications with long term infection: • TSS (immunologic) • Quartan malaria nephropathy (immunologic)
Factors that may affect prognosis • ØMultiple complications • Ø20% of RBC contain mature parasites • Ø5% of neutrophils contain pigment • Concomitant Gram-negative bacteria infection • Cerebral symptoms
Diagnosis • Microscopy: Thick and thin films (variation in level of parasitemia with time, examine 8 hourly x 3 days, during and between fever). Skills and expertise required. • Buffy coat method (more sensitive, requires fluorescent microscopy) • P. Falciparum dipstick antigen capture assay (sen & spe 75%-95%) • Serology tests (ELISA): antibody available after 8-10 days and remains 10 or more years • PCR: highly specific but requires special labs.
Diagnosis----- • CBC findings: Anemia Reticulocytosis Transient leukocytosis (during paroxysms) Subsequent leukopenia, with relative elevated large mononuclear cells • LFT may be abnormal
Differential Diagnosis Causes of fever, anemia, splenomegally, hepatomegally, etc should be excluded. Malaria can mimic many diseases depending on the complications and stage of presentation ØInfluenza • ØDengue Fever & Dengue Hemorrhagic Fever • ØTyphoid • ØUTI • ØHepatitis • ØLeptospirosis • ØRelapsing fever • Pneumonia, etc
Differential Diagnosis----- • > Sepsis • ØPneumonia • ØPharyngitis • Gastroenteritis
TreatmentModality • Always suspect malaria for fever in an endemic area or after visit to an endemic area • Single negative Laboratory test does not rule out the disease • Think about the type of plasmodium and aim at eradication treatment • Think about drug resistance • Chloroquine is no longer used for treatment in many areas due to resistance • For P. Vivax and P. Ovale always give eradication treatment
TreatmentModality----- • Drug side effects and appropriateness to patient group • Talk about prevention at each patient visit to emphasize the role of the individual and the community
Selected Drugs Chloroquine: • Indications- Chloroquine sensitive all forms except resistant P. falciparum and P. Vivax • Dosage: Oral-25mg/kg base in divided doses: typical 600mg start, 300mg after 6-8 hours, 300mg every day for 2 more days IM or slow IV-10mg/kg over 8 hours, • then 5mg/kg q 8 hours x 3 doses • then oral dosing until a total of 25mg/kg is given
Chloroquine---- • Side effects: Impaired hearing, psychosis, convulsions, blood dyscrasias, skin allergy, hypotension, haemolysis in G6PD. Long term use may cause dose dependent retinopathy, ototoxicity and myopathy. • Pregnancy: not contraindicated • Children: not contraindicated
Mefloquine hydrochloride • Indications-Chloroquine resistant malaria (Treatment) • Dosage: Oral-20-25mg/kg base single dose or in divide doses Typical 750mg start, then 500mg after 6- 12 hours • Side effects: Cardiac conduction problems (prolongation of QT interval), liver effect, ophthalmopathy, neuropsychiatric symptoms (rare)
Mefloquine----- • Contraindications: Cardiac conduction problems, Neuropsychiatric problems (including epilepsy, depression, psychosis etc), Liver dysfunction, Concurrent use of quinine, quinidine, or halofantrin (allow 12 hours after these drugs b/4 mefloquine, and allow 13-26 days (the elimination ½ life) after mefloquine before these drugs) • Pregnancy: Not contraindicated • Children: Can be given to children above 12 weeks
Primaquine • Indications-P.vivax, P.Ovale, P. Falciparum (gametocyte specific, active against hypnozoids) • Dosage: 15mg daily for 14-21 days • Side effects: Haemolysis in G6PD deficiency, GIT disturbance, headache, dizziness • Contraindications: Autoimmune dx, pregnancy, quinine use, G6PD deficiency (all Africans, E. Asians and Mediterranean should have blood check for G6PD before medication)
Fansidar • Indication-susceptible P. Falciparum, low efficacy against P. vivax, P ovale and P malariae • Dosage: Each tablet contains 25mg pyrimethamine and 500mg sulfadoxine Typical oral 3 tablets one time • Side effects: Erytheme multiforme and other sulfonamide reactions, Kernicterus in the new born, haemolysis in G6PD deficiency
Fansidar---- • Caution: Liver and renal impairment, G6PD def, children • Pregnancy: contraindicated • Children: with caution
Doxycycline • Indications-all plasmodium types • Dosage: Oral 200mg daily for 7 days (note milk reduces absorption) • Side effects: GIT symptoms, Oesophageal irritation (take with food and water), Candidal vaginitis, photosensitivity (use sunscreens), chemical hepatitis. • Contraindication: Pregnancy, children below 8 years, hepatic dysfunction
Quinine • Indication- Life threatening malaria (including cerebral malaria), multidrug resistant malaria • Dosage: IV loading 20mg/kg over 4 hours Then 10mg/kg over 4 hours at 8-12 hourly interval until patient can swallow tablets Oral-600mg tid x 7 days Followed by fansidar 3 tablets one dose or doxycycline
Quinine----- • Side effects: Cinchonism (headache, nausea, dizziness, visual disturbances, tinnitus) Severe reaction include: fever, deafness, visual effects (blindness, optic atrophy, diplopia, scotomas, retinal vessel spasticity, etc). Vertigo, confusion, seizures may occur. Cardiac conduction abnormalities(do not give with mefloquine, halofantrin), thrombophlebitis. • Drug interactions: Aluminium containing antacids, digoxin, anticoagulants and cimetidine.
Quinine----- • Contraindications: Cardiac conduction problems especially prolonged QT interval or polymorphic ventricular tarchycardia. • Pregnancy: not contraindicated • Children: not contraindicated
Artemisinin and its derivatives • Indications- All malaria parasites. Most rapidly acting blood schizonticide. No resistance reported as yet. Used for quinine resistant p falciparum. Can not be used for prophylaxis (short ½ life) • Dosage: oral/IV artesunate 4mg/kg/d for 3 days, followed by mefloquine. IM artemether 3.2mg/kg, then 1.6mg/kg daily, followed by mefloquine
Artemisinin and its derivatives- • Side effects: GIT symptoms, fever, headache and pruritus. Study suggest embryotoxicity and neurotoxicity (not recorded in humans) • Pregnancy: contraindicated
Preventing vector bite • Repellant: Deet (N, N-diethyl-3-methylbenzamide) used on the exposed parts of the body may be effective for 2-4 hours. • Risk: there is a slight risk of toxic encephalopathy with the use of deet. (apply sparingly on the exposed parts only and wash off when indoors)
Prophylaxis • For prophylaxis, malaria endemic areas are grouped into • Regions with chloroquine sensitive P falciparum and • Regions with chloroquine resistance P falciparum • Regions with chloroquine sensitive P falciparum Central America west of panama canal, the Caribbean, North Africa, and parts of the middle East
Prophylaxis----- Chloroqiune phosphate 300mg base/week plus or minus proguanil 100mg daily is recommended in these areas • Regions with chloroquine resistance P falciparum All other areas of the endemic areas belong to this region. Mefloquine 250mg weekly (1 week b/4 entering the area and 4 weeks after leaving the area) Or
Prophylaxis---- Doxycycline 100mg daily (2 days b/4 entering the area and 4 weeks after leaving the area) Or Malarone (atovaquone 250mg + Proguanil 100mg) 1 tablet daily (1 day b/4 entering the area and 1 week after leaving