Download
1 / 1
10 likes | 118 Views
Improving Kidney Exchange with Compatible Pairs Do One Transplant, Get One Free Karna Mital , Duke University. The National Problem of Kidney Failure. Contribution – Incorporating Compatible Pairs. Results. Conclusion and Applications.

E N D
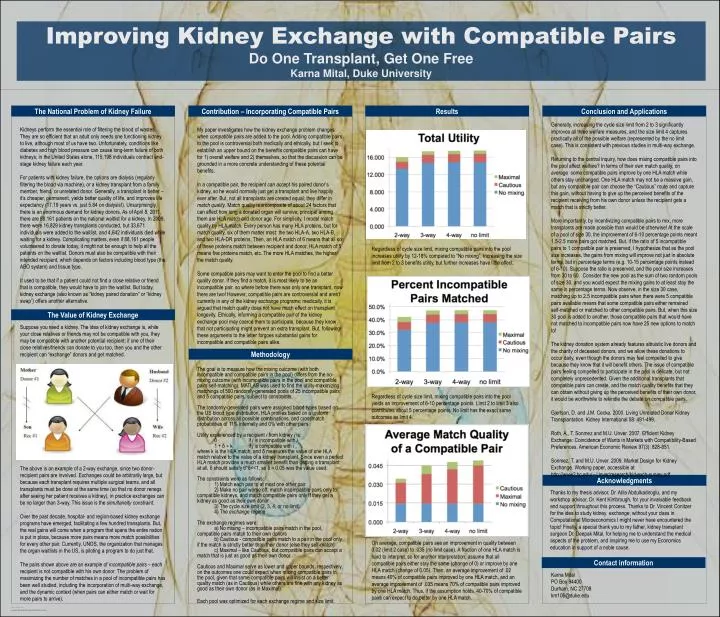
Improving Kidney Exchange with Compatible Pairs Do One Transplant, Get One FreeKarnaMital, Duke University The National Problem of Kidney Failure Contribution – Incorporating Compatible Pairs Results Conclusion and Applications Generally, increasing the cycle size limit from 2 to 3 significantly improves all three welfare measures, and the size limit 4 captures practically all of the possible welfare (represented by the no limit case). This is consistent with previous studies in multi-way exchange. Returning to the central inquiry, how does mixing compatible pairs into the pool affect welfare? In terms of their own match quality, on average some compatible pairs improve by one HLA match while others stay unchanged. One HLA match may not be a massive gain, but any compatible pair can choose the “Cautious” route and capture this gain, without having to give up the perceived benefits of the recipient receiving from his own donor unless the recipient gets a match that is strictly better. More importantly, by incentivizing compatible pairs to mix, more transplants are made possible than would be otherwise! At the scale of a pool of size 30, the improvement of 6-10 percentage points meant 1.5-2.5 more pairs got matched. But, if the ratio of 5 incompatible pairs to 1 compatible pair is preserved, I hypothesize that as the pool size increases, the gains from mixing will improve not just in absolute terms, but in percentage terms (e.g. 10-15 percentage points instead of 6-10). Suppose the ratio is preserved, and the pool size increases from 30 to 60. Consider the new pool as the sum of two random pools of size 30, and you would expect the mixing gains to at least stay the same in percentage terms. Now observe, in the size 30 case, matching up to 2.5 incompatible pairs when there were 5 compatible pairs available means that some compatible pairs either remained self-matched or matched to other compatible pairs. But, when this size 30 pool is added to another, those compatible pairs that would have not matched to incompatible pairs now have 25 new options to match to! The kidney donation system already features altruistic live donors and the charity of deceased donors, and we allow these donations to occur daily, even though the donors may feel compelled to give because they know that it will benefit others. The issue of compatible pairs feeling compelled to participate in the pool is delicate, but not completely unprecedented. Given the additional transplants that compatible pairs can create, and the match quality benefits that they can obtain without giving up the perceived benefits of their own donor, it would be worthwhile to rekindle the debate on compatible pairs. Gjertson, D. and J.M. Cecka. 2000. Living Unrelated Donor Kidney Transplantation. Kidney International 58: 491-499. Roth, A., T. Sonmez and M.U. Unver. 2007. Efficient Kidney Exchange: Coincidence of Wants in Markets with Compatibility-Based Preferences. American Economic Review 97(3): 828-851. Sonmez, T. and M.U. Unver. 2009. Market Design for Kidney Exchange. Working paper, accessible at http://www2.bc.edu/∼Unver/research/kid-exch-survey.pdf . Kidneys perform the essential role of filtering the blood of wastes. They are so efficient that an adult only needs one functioning kidney to live, although most of us have two. Unfortunately, conditions like diabetes and high blood pressure can cause long-term failure of both kidneys; in the United States alone, 115,198 individuals contract end-stage kidney failure each year. For patients with kidney failure, the options are dialysis (regularly filtering the blood via machine), or a kidney transplant from a family member, friend, or unrelated donor. Generally, a transplant is better – it’s cheaper, permanent, yields better quality of life, and improves life expectancy (17.19 years vs. just 5.84 on dialysis!). Unsurprisingly, there is an enormous demand for kidney donors. As of April 8, 2011, there are 88,161 patients on the national waitlist for a kidney. In 2009, there were 16,829 kidney transplants conducted, but 33,671 individuals were added to the waitlist, and 4,642 individuals died while waiting for a kidney. Complicating matters, even if 88,161 people volunteered to donate today, it might not be enough to help all the patients on the waitlist. Donors must also be compatible with their intended recipient, which depends on factors including blood type (the ABO system) and tissue type. It used to be that if a patient could not find a close relative or friend that is compatible, they would have to join the waitlist. But today, kidney exchange (also known as “kidney paired donation” or “kidney swap”) offers another alternative. My paper investigates how the kidney exchange problem changes when compatible pairs are added to the pool. Adding compatible pairs to the pool is controversial both medically and ethically, but I seek to establish an upper bound on the benefits compatible pairs can have for 1) overall welfare and 2) themselves, so that the discussion can be grounded in a more concrete understanding of these potential benefits. In a compatible pair, the recipient can accept his paired donor’s kidney, so he would normally just get a transplant and live happily ever after. But, not all transplants are created equal; they differ in match quality. Match quality is a composite of about 24 factors that can affect how long a donated organ will survive; principal among them are HLA match and donor age. For simplicity, I model match quality by HLA match. Every person has many HLA proteins, but for match quality, six of them matter most: the two HLA-A, two HLA-B, and two HLA-DR proteins. Then, an HLA match of 6 means that all six of these proteins match between recipient and donor, HLA match of 5 means five proteins match, etc. The more HLA matches, the higher the match quality. Some compatible pairs may want to enter the pool to find a better quality donor. If they find a match, it is most likely to be an incompatible pair, so where before there was only one transplant, now there are two! However, compatible pairs are controversial and aren’t currently in any of the kidney exchange programs; medically, it is argued that match quality does not have much effect on transplant longevity. Ethically, informing a compatible pair of the kidney exchange pool may coerce them to participate, because they know that not participating might prevent an extra transplant. But, following these arguments to the letter forgoes substantial gains for incompatible and compatible pairs alike. The goal is to measure how the mixing outcome (with both incompatible and compatible pairs in the pool) differs from the no-mixing outcome (with incompatible pairs in the pool and compatible pairs self-matching). MATLAB was used to find the utility-maximizing matchings of 500 randomly-generated pools of 25 incompatible pairs and 5 compatible pairs, subject to constraints. The randomly-generated pairs were assigned blood types based on the US blood type distribution, HLA profiles based on a uniform distribution across all possible combinations, and crossmatch probabilities of 11% internally and 0% with other pairs. Utility experienced by a recipient i from kidney j is: 0 if j is incompatible with i 1 + δ ∗ k if j is compatible with i , where k is the HLA match, and δ measures the value of one HLA match relative to the value of a kidney transplant. Since even a perfect HLA match provides a much smaller benefit than getting a transplant at all, δ should satisfy 6*δ<<1, so δ = 0.05 was the value used. The constraints were as follows: 1) Match each pair to at most one other pair 2) Make no pair worse off: match incompatible pairs only to compatible kidneys, and match compatible pairs only if they get a kidney as good as their own donor 3) The cycle size limit (2, 3, 4, or no limit) 4) The exchange regime The exchange regimes were: a) No mixing – incompatible pairs match in the pool, compatible pairs match to their own donors b) Cautious - compatible pairs match to a pair in the pool only if the match is strictly better than their donor (else they self-match) c) Maximal – like Cautious, but compatible pairs can accept a match that is just as good as their own donor Cautious and Maximal serve as lower and upper bounds, respectively, on the outcomes one could expect when mixing compatible pairs in the pool, given that some compatible pairs will insist on a better quality match (as in Cautious) while others are fine with any kidney as good as their own donor (as in Maximal). Each pool was optimized for each exchange regime and size limit. Regardless of cycle size limit, mixing compatible pairs into the pool increases utility by 12-18% compared to “No mixing”. Increasing the size limit from 2 to 3 benefits utility, but further increases have little effect. The Value of Kidney Exchange Suppose you need a kidney. The idea of kidney exchange is, while your close relatives or friends may not be compatible with you, they may be compatible with another potential recipient; if one of their close relatives/friends can donate to you too, then you and the other recipient can “exchange” donors and get matched. Methodology Regardless of cycle size limit, mixing compatible pairs into the pool yields an improvement of 6-10 percentage points. Limit 2 to limit 3 also contributes about 5 percentage points. No limit has the exact same outcomes as limit 4. The above is an example of a 2-way exchange, since two donor-recipient pairs are involved. Exchanges could be arbitrarily large, but because each transplant requires multiple surgical teams, and all transplants must be done at the same time (so that no donor renegs after seeing her patient receives a kidney), in practice exchanges can be no larger than 3-way. This issue is the simultaneity constraint. Over the past decade, hospital- and region-based kidney exchange programs have emerged, facilitating a few hundred transplants. But, the real gains will come when a program that spans the entire nation is put in place, because more pairs means more match possibilities for every other pair. Currently, UNOS, the organization that manages the organ waitlists in the US, is piloting a program to do just that. The pairs shown above are an example of incompatiblepairs – each recipient is not compatible with his own donor. The problem of maximizing the number of matches in a pool of incompatible pairs has been well studied, including the incorporation of multi-way exchange, and the dynamic context (when pairs can either match or wait for more pairs to arrive). Acknowledgments Thanks to my thesis advisor, Dr. AtilaAbdulkadiroglu, and my workshop advisor, Dr. Kent Kimbrough, for your invaluable feedback and support throughout this process. Thanks to Dr. Vincent Conitzer for the idea to study kidney exchange; without your class in Computational Microeconomics I might never have encountered the topic! Finally, a special thank you to my father, kidney transplant surgeon Dr. Deepak Mital, for helping me to understand the medical aspects of the problem, and inspiring me to use my Economics education in support of a noble cause. On average, compatible pairs see an improvement in quality between 0.02 (limit 2 case) to .035 (no limit case). A fraction of one HLA match is hard to interpret, so for another interpretation, assume that all compatible pairs either stay the same (change of 0) or improve by one HLA match (change of 0.05). Then, an average improvement of .02 means 40% of compatible pairs improved by one HLA match, and an average improvement of .035 means 70% of compatible pairs improved by one HLA match. Thus, if the assumption holds, 40-70% of compatible pairs can expect to do better by one HLA match. Contact information KarnaMital PO Box 94400 Durham, NC 27708 km106@duke.edu