Download
1 / 15
150 likes | 288 Views
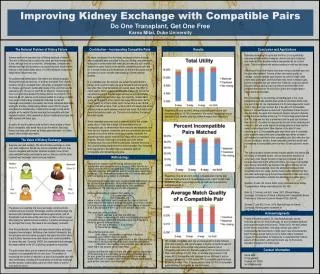
Kidney Exchange Enrichment. Michael Levy David Flatow. The Problem. End Stage Renal Disease (ESRD) is a fatal disease unless treated with dialysis or kidney transplantation (preferred method) 86,000 patients on the waiting list (Jan ‘09-Dec ’09) Median wait time for transplant: 4 years

E N D
Kidney Exchange Enrichment Michael Levy David Flatow
The Problem • End Stage Renal Disease (ESRD) is a fatal disease unless treated with dialysis or kidney transplantation (preferred method) • 86,000 patients on the waiting list (Jan ‘09-Dec ’09) • Median wait time for transplant: 4 years • 4,600 patients died • 34,000 new patient registrations • 10,400 transplants of cadaver kidneys and 6,400 transplants of kidneys from living donors • Want to alleviate this shortage and improve patient welfare
The Problem (Cont’d) • Two genetic characteristics play key roles in the success of a kidney transplant • ABO blood-type • Type O can only receive type O • HLA (tissue) type • Mismatch decreases likelihood of successful graft (Opelz, 1997) • The presence of antibodies, called a positive crossmatch, effectively rules out transplantation
The Problem (Cont’d) • 1/3 of O donor kidneys go to non-O recipients • 1/3 of A recipients have O donors • ½ of B recipients have O donors
The Status Quo • Transplants from live donors generally have a higher chance of success than those from cadavers • A patient identifies a healthy, willing, feasible donor and the transplant it is carried out • Other types of exchanges • paired exchange • indirect exchange (list exchange) • market exchange • Can we do better?
Top Trading Cycle with Chains (TTCC) • Each remaining active patient points to his most preferred remaining unassigned kidney or to the wait-list option, whichever is more preferred • There is either a cycle, or a chain, or both. • Proceed to Step 3 if there are no cycles. Otherwise, remove all patients in a cycle together with their assignments. • Each remaining patient points to his top choice among remaining kidneys. Locate all cycles and remove them. Repeat until no cycle exists. • If there are no pairs left, we are done. Otherwise, remove only one of the chains with the chain selection rule. • After a w-chain is selected, new cycles may form. Repeat Steps 2 and 3 with the remaining active patients and unassigned kidneys until no patient is left.
Rationality • Patient Rationality (Roth et al, 2004) • depends HLA mismatches ( x) and donor age ( y) • “rational” u(x,y)=0.514x - y/10 • “cautious” IRs prefer other compatible Ds to his own only if they are more than an equivalent of one HLA mismatch better • Want to redefine “cautious” and explore benefits of incentive schemes of entering the market • Under Roth’s definition of “cautious”, an IR would join the kidney exchange even if they had a compatible D
Rationality (Cont’d) • Compatible pairs do not join the exchange (Gentry et al, 2007) • Participation of compatible pairs can double the match rate for incompatible pairs (Gentry et al, 2007) • Reflects preferences for a related donor, time constraints, and incomplete information • How can we get more compatible people to join?
Rationality (Cont’d) • “Opt Out” versus “Opt In” policy • Put everyone into the system • Can always leave at no cost • Updating preferences with possible matches • “Completing” their information • Updating preferences with possible matches • Less repugnant than “Opt Out”
Multiple Donors • Single Donors • Currently, each IR brings a single D to the exchange (Roth et al, 2004) • Optimizing which donor to bring • Want to allow each IR to bring multiple Ds • Only one donates (Roth et al, 2006) • Possibly multiple donate • Any D in a cycle or starts an altruistic chain donates • A certain number donates to an IR or the waitlist • All donate to an IR or the waitlist
Multiple Donors (Cont’d) • Roth et al, 2006 demonstrated efficiency gains when only one of your multiple Ds donates • Multiple people donating will create more efficiency • Is it too repugnant? • Are there incentives to bring less people? • Are there issues with reneging? • Conjecture: Having multiple Ds donate does not improve the kidney you receive compared to when only one of your multiple Ds donates
Multiple Donors (Cont’d) • Should people with more Ds donating get preferential treatment? • Do we lose stability? • Too repugnant? • Overcome the conjecture? • Multiple donating comes with several caveats • Concentrated risk • Logistical concerns • Stop people from incrementing their donor set?
Other Considerations • Stricter blood type matching • “Save” O kidneys for O patients, A for As, etc. • Donor Swapping • Your D donates to someone in exchange for their D to be paired with you • Altruistic Donors • Can we increase the amount of altruism? • Non-Simultaneous Extended Altruistic Donor Chains speak well about reneging