Download
1 / 24
240 likes | 259 Views
AJR 2006; 186:1103-1112. Mimics of Appendicitis, Alternative Nonsurgical Diagnosis with Sonography and CT. Adriaan C. van Breda Vriesman, Julien B. C. M. Puylaert AJR:186, April 2006. 2007.4.19. 8:00am MRI 會議室 Presented by int. 黃子青 Supervisor: Pro. 姚維仁. Outline.

E N D
AJR 2006; 186:1103-1112 Mimics of Appendicitis, Alternative Nonsurgical Diagnosis with Sonography and CT Adriaan C. van Breda Vriesman, Julien B. C. M. Puylaert AJR:186, April 2006 2007.4.19. 8:00am MRI會議室 Presented by int. 黃子青 Supervisor: Pro. 姚維仁
Outline • Abstract • Introduction • Normal and Inflamed Appendix • Nonsurgical Mimics of Appendicitis
Abstract • Objective • Imaging features • Nonsurgical disorders + Clinical signs of appendicitis • Conclusion: • Sonographic & CT features Self-limiting or be treated conservatively avoid nontherapeutic appendectomy and unnecessary hospitalization
Normal Appendix • Outer diameter of the appendix <6-7 mm
Normal Appendix • Air-filled nondistended appendix
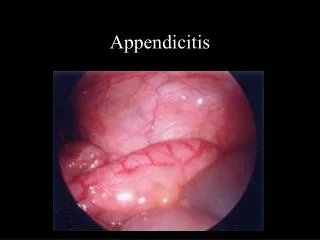
Inflamed Appendix hyperechoic inflamed fat (arrowheads) hypervascularity of appendiceal wall
Inflamed Appendix fluid-filled distended appendix Extramural changes with fat stranding on CECT
Inflamed Appendix • Signs of inflammation • Appendicolith • Cecal apical thickening • Color Doppler sonography: hypervascularity of the appendix wall
Nonsurgical Mimics of Appendicitis • Mesenteric adenitis • Bacterial ileocecitis • Epiploic Appendagitis • Omental infarction • Colonic Diverticulitis • Ileocecal Crohn's Disease • Ileocecal Intussusception • Pelvic Inflammatory Disease • Urolithiasis • Rectus sheath hematoma
Nonsurgical Mimics of Appendicitis • Mesenteric adenitis : 2nd RLQ pain • inflammation (R’t) mesenteric lymph nodes • Normal appendix • self-limiting clustered adenopathy
Nonsurgical Mimics of Appendicitis • Bacterial ileocecitis • Yersinia, Campylobacter, or Salmonella spp • Image: • Mural thickening of the terminal ileum and cecum • No inflammation of the surrounding fat • Moderate mesenteric adenopathy. Infectious ileocecitis caused by Yersinia, Campylobacter, and Salmonella: Clinical, radiological and US findings. Eur Radiol 1997; 7:3–9
Bacterial Ileocecitis • terminal ileum and cecum :moderate mural thickening • surrounded by normal noninflamed fat 39 y/o, male
Epiploic Appendagitis • Epiploic appendage: torsion or 2° inflammation • self-limiting disease hyperechoic inflamed fatty mass fatty lesion contains hyperdense ring Colon
Omental infarction • R’t omentum: infarcted fatty tissue inflamed intraperitoneal fat omental fat: cakelike, slightly dense inflamed
Differential Diagnosis • ovoid inflamed fatty mass • Shape and size of lesion suggest epiploic appendagitis • No hyperdense ring D.D.: Epiploic Appendagitis Omental infarction All benign dz
Colonic Diverticulitis cecal wall : fat stranding inflamed cecal diverticulum surrounded by hyperechoic fat.
inflamed cecal diverticulum (arrow) with fecalith surrounded by fat stranding.
Ileocecal Crohn's Disease terminal ileum: transmural wall thickening surrounding fat : hyperechoic inflammatory changes
Ileocecal Crohn's Disease • wall thickening and luminal narrowing of terminal and preterminal ileum (arrowheads) with regional fat stranding.
Ileocecal Intussusception • Targetlike mass , distal ileum into cecum
Pelvic Inflammatory Disease TVS: CECT enlarged ovary free pelvic fluid
Rectus sheath hematoma • painful palpable mass under anticoagulant therapy Fluid-fluid level partly hyperdense mass
Nonsurgical Mimics of Appendicitis • Mesenteric adenitis, Bacterial ileocecitis , Epiploic Appendagitis , Omental infarction, Colonic Diverticulitis, Ileocecal Crohn's Disease , Ileocecal Intussusception , Pelvic Inflammatory Disease, Urolithiasis, Rectus sheath hematoma • correct imaging diagnosis • prevents an unnecessary operation or hospitalization.