Download
1 / 66
670 likes | 693 Views
Explore the characteristics, spread, and effects of Mycobacterium tuberculosis, including its epidemiology, modes of spread, pathogenesis, and clinical outcomes. Learn about primary and secondary TB, granuloma formation, and the impact of HIV co-infection.

E N D
Introduction • Chronic granulomatous inflammation. • Granuloma-granule like lesion • Epithelioidcells,giantcells,necrosis & fibrosis. • Factors favouring-poorly digestible irritant -cell mediated immunity.
Causative organism • Koch’s bacillus • Pathogenic strains -tuberculosis -bovis -avium -murine
Atypical mycobacteria-photochromogens -scotochromogens -nonphotochromogens -rapid growers. • Lesions caused-pulmonary -abscesses -lymphadenitis -bacteremia -ulcers -longer,thicker, more coarsely beaded,bent.
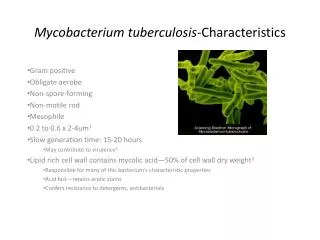
Mycobacterium TB • Slender, strictly aerobic rods • Waxy cell wall of mycolic acid • Methods of demonstration- -Ziehl-Neelsen method -fluorescent dye -culture-LJ medium -guinea pig inoculation
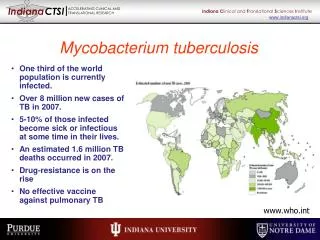
Epidemiology • 8 to 10 million cases/year • Leading infectious cause of death after HIV • Incidence increased after emergence of HIV • Flourishes-poverty,crowding,chronic debilitating illnesses,immunosuppression.
Modes of spread • Inhalation-airborne droplets • Ingestion-bovine TB • Inoculation - • Trans-placental- ?
Pathogenesis • Inhalation of tubercle bacilli • Mannose receptor of macrophage binds lipoarabinomannan on bacteria • Unchecked proliferation-?reasons • TH1 response-bactericidal macrophages • IFN gamma induces NO formation • TH1 response orchestrates formation of granuloma & caseous necrosis.
IFN gamma activates macrophages producing TNF • TNF recruits monocytes –epithelioid & giant cells • In summary- central role of TH1 -confers immunity -hypersensitivity- granuloma -caseation.
No infection 78% Exposure (close contact) Primary active TB 5% Continued latent TB Infection 22% Secondary TB 10%/lifetime Latent TB 95% HIV infection 10%/year Outcome of Exposure to M. tuberculosis
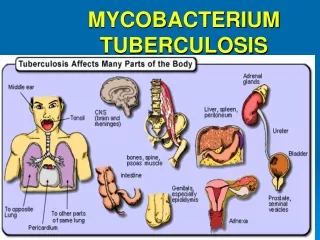
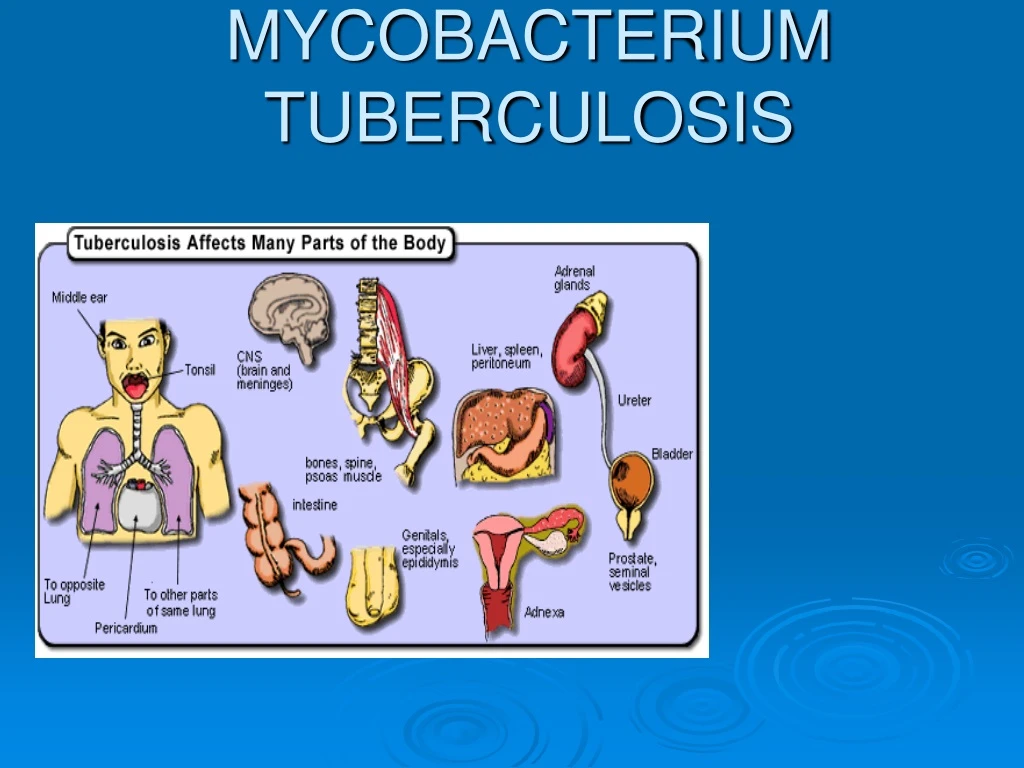
Primary tuberculosis: initial infection, usually in children - Ghon complex - subpleuralgranuloma + granulomatous hilar lymph node infection • Secondary tuberculosis: mostly in adults as a reactivation of previous infection (or reinfection)- granulomatous inflammation is much more florid and widespread - Typically, the upper lung lobes are most affected • Miliary tuberculosis- small millet seed (1-3 mm) sized granulomas
Tubercle • Caseous/non-caseous focus of inflammation consisting of: • Epitheloid cells • Langhan’s giant cells • Surrounded by lymphocytes and fibroblasts. • Fate of the tubercles– cold abscess, sinuses, coalesce to form large tubercles, dystrophic calcification.
Tubercle bacilli Lymphocyte Giant cells Fully activated macrophage Partially activated macrophage
Types PRIMARY TB: -previously unexposed, unsensitized -exogenous source of infection -primary or Ghon complex a)primary Ghon focus b)lymphatic c)lymph node
2.PROGRESSIVE PRIMARY TB -resemble acute bacterial pneumonia -lower & middle lobe consolidation -hilaradenopathy -pleural effusion -cavitation rare 3.PRIMARY MILIARY TB -TB meningitis,miliary TB.
Fate of primary TB In 95% of cases healing by fibrosis -calcification -Ranke complex (X-ray)
SECONDARY TB: • Previously sensitized. • Re-activation of dormant bacilli • Re-infection TB A)high dose of virulent bacilli B)primary immunity wanes off.
Morphology • Initial lesion: -small focus(<2cm) of consolidation within 1-2 cms of apical pleura. -sharply circumscribed,firm ,grey-white to yellow areas with central caseation & peripheral fibrosis. -Because of good hypersensitivity ,walling off occurs.-FIBROCASEOUS SCARS.
PROGRESSIVE PULMONARY TB: -Elderly,Immunosuppression -apical lesion enlarges -erosion into a bronchus -ragged irregular cavity,poorly walled off • Cavities may remain or collapse • spread-airways,lymphatic,hematogenous
Miliary TB MILIARY PULMONARY DISEASE • Through lymphatics to rt.side of heart and pulmonary arteries. • Small(2mm) yellow white consolidation scattered throughout lung. -Pleural spread -effusion -empyema -obliterative fibrous pleuritis.
SYSTEMIC MILIARY DISEASE Hematogenous dissemination Organs affected: liver, spleen, kidneys, adrenals, bone marrow. Multiple tiny tubercles –grey white to yellow,
Endobronchial, endotracheal and laryngeal TB: • Infective material spread through lymphatics • Expectorated infectious material. • Mucosa studded with minute granulomas • Isolated organ TB & lymhadenitis are other forms of TB.
TB & HIV • Increased incidence in HIV • CD4 count >300 -secondary TB • CD4 count <200 -progressive primary • Sputum smear –ve,TUBERCULIN test –ve & rare formation of granulomas. • Sheets of foamy histiocytes packed with bacilli.
In AIDS ,MAC causes widely disseminated infections • Proliferation in lungs & GIT • Fever, drenching night sweats & weight loss. • Enlargement of lymph nodes, liver & spleen • Granulomas, lymphocytes & tissue destruction are rare.
Diagnosis History Clinical examination X-ray examination Smear for AFB Culture PCR-
Laboratory diagnosis of tuberculosis Proper collection of samples • Sputum – the commonest SPOT-EARLY MORNING-SPOT • Well-coughed-up mucoid- collected into a wide mouthed waxed carton / plastic container with a lid • Examined as quickly as possible
MYCOBACTERIUM • Aerobic bacilli –non spore forming -non motile • Cell wall –rich in lipids • Acid-fast bacilli • Chains of cells in smears made from in vitro-grown colonies often form distinctive serpentine cords
Digestion & decontamination • Samples that are contaminated with normal flora- sputum,gastric aspirates, urine • Treated with acid alkali or detergent • Kill normal flora & allow mycobacteria to survive • Mucolytic • Weak- NaOH , N-acetylcysteine, oxalic acid • Modified Petroffs – all samples Oxalic acid for – Bronchoalveolar lavage.
Newer Techniques in the identification of M tbc • PCR Polymerase chain reaction • Quantiferon Assay • HPLC- Fatty acid profile