Download
1 / 2
20 likes | 120 Views
Med Profile Tab – “One Source of Truth”. ACCESSING THE “One Source of Truth” Physicians : through “Admission or Post-Op Order Sets” or Placing a “Medication Reconciliation Order” Nurses : Medication Reconciliation PowerForm through Task List or Ad Hoc Charting

E N D
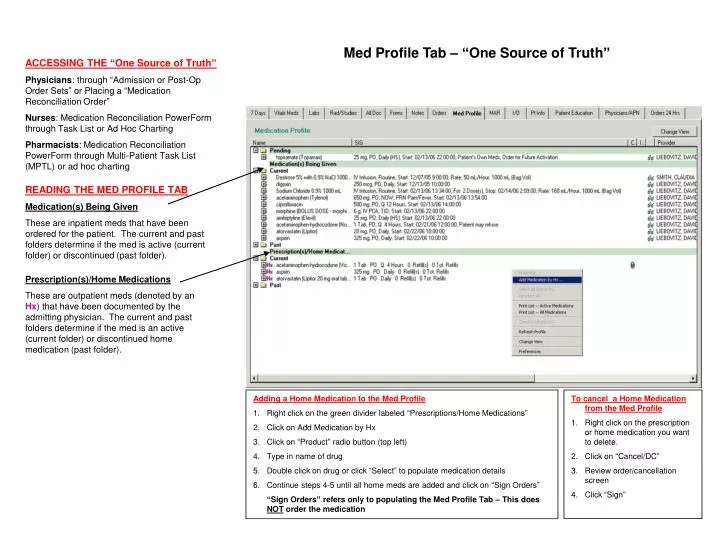
Med Profile Tab – “One Source of Truth” ACCESSING THE “One Source of Truth” Physicians: through “Admission or Post-Op Order Sets” or Placing a “Medication Reconciliation Order” Nurses: Medication Reconciliation PowerForm through Task List or Ad Hoc Charting Pharmacists: Medication Reconciliation PowerForm through Multi-Patient Task List (MPTL) or ad hoc charting READING THE MED PROFILE TAB Medication(s) Being Given These are inpatient meds that have been ordered for the patient. The current and past folders determine if the med is active (current folder) or discontinued (past folder). Prescription(s)/Home Medications These are outpatient meds (denoted by an Hx) that have been documented by the admitting physician. The current and past folders determine if the med is an active (current folder) or discontinued home medication (past folder). • Adding a Home Medication to the Med Profile • Right click on the green divider labeled “Prescriptions/Home Medications” • Click on Add Medication by Hx • Click on “Product” radio button (top left) • Type in name of drug • Double click on drug or click “Select” to populate medication details • Continue steps 4-5 until all home meds are added and click on “Sign Orders” • “Sign Orders” refers only to populating the Med Profile Tab – This does NOT order the medication • To cancel a Home Medication from the Med Profile • Right click on the prescription or home medication you want to delete. • Click on “Cancel/DC” • Review order/cancellation screen • Click “Sign”
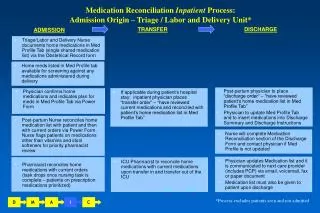
Roles and Responsibilities for Medication Reconciliation • ADMISSION • Physicians document home medications in Med Profile Tab by placing a “Medication Reconciliation” order or through an Admission or Post-OP Order Set; if home meds already there, confirm accuracy of home med list • Nurses verify home medications with patient, add any new information to the med profile, reconcile home medications with inpatient orders and document all information above in the Nursing – Medication Reconciliation PowerForm • Pharmacists reconcile home medications with inpatient orders and document in the Pharmacy – Medication Reconciliation PowerForm • Note: For ICU patients, ICU pharmacists will perform medication reconciliation – Steps 2 and 3. • TRANSFER • All Physiciansplace a “medication reconciliation order” at transfer. This order signifies that the physician has reviewed the current medications and reconciled with patient’s home medication list in Med Profile Tab. • In ICU, ICU Pharmacists reconcile home medications with current medications upon transfer in and transfer out of the ICU • DISCHARGE • Physicians place a “Discharge – Medication Reconciliation Order” and update the patient’s home medication list prior to discharge • Physicians can insert home medications from the Med Profile Tab into the Discharge Summary and Discharge Instructions (Please confirm medication list is translated into patient-friendly language i.e., change BID to 2 times a day) • Physicians communicate the most current medication list to next care provider and give patient updated home medication list in patient friendly language • Nurses complete discharge note and verify updated home med list has been given to patient and is consistent with discharge instructions Medication Reconciliation National Patient Safety Goal #8: To accurately and completely reconcile medications across the continuum of care.