Download
1 / 40
470 likes | 739 Views
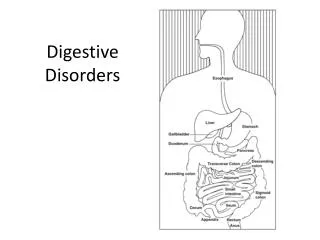
Digestive Disorders. Stomach. Digestion occurs in 2 phases Cephalic phase Food traveling down esophagus & into the stomach HCl acid & digestive juices are secreted in stomach Gastric phase When food passes the cardiac sphincter Stretching the stomach mucosa stimulates gastrin

E N D
Stomach • Digestion occurs in 2 phases • Cephalic phase • Food traveling down esophagus & into the stomach • HCl acid & digestive juices are secreted in stomach • Gastric phase • When food passes the cardiac sphincter • Stretching the stomach mucosa stimulates gastrin • (What does gastrin do?)
Gastric Juice • pH of .9-1.5 • Contains • HCl • Pepsin (What does it help break down?) • Intrinsic Factor (What does it help absorb?) • Proteolytic enzymes • Mixes with food to form what?
Large Intestines • There are several bacteria that live in the large intestines • Escherichia coli • Enterobacteraerogenes • Clostridium welchii • Lactobacillus bifidus • What are their purposes?
Functions of the Liver • Filters & detoxifies blood • Removes foreign substances such as drugs, ETOH, other toxins • Removes natural occurring ammonia from body fluids & converts it to urea (then what does it do with it?) • Produces Vitamin A • Plasma proteins • Non-essential amino acids • Makes bile • Converts glucose to glycogen • Stores fats & sugars
Pancreas • Exocrine & endocrine tissue • Secretes 1000 ml of digestive enzymes / day • Divided into 3 sections. What are they?
Appendicitis • Most common between puberty & age 25 • Men/women are equal • Old thought was that fesces caused an obstruction • Now the belief that there is a mucosal ulceration first that may be caused by a virus
Progression • Ulceration of the mucosal lining • Inflammation & temporary obstruction of the appendix • Obstruction usually by fecal matter • Mucus outflow is blocked & the appendix becomes distended • Pressure within the appendix increases & contracts • Bacteria multiply & inflammation continue to increase; affecting blood flow to organ & causing severe abdominal pain
Appendicitis cont • What are some complications? • Infection & rupture • Peritonitis (most common & most dangerous) • Patients present: • Anorexia • N & V • Low grade fever • Rebound tenderness (where?)
Tests • WBC (may be moderately high) • Abdominal X-ray with contrast • Failure of contrast to enter the appendix shows obstruction • Other conditions with similar symptoms to rule out: • Cystitis • Ovarian cyst • Pancreatitis • Diverticultis • Gastritis
Treatment • Surgical Removal • Gastric intubation • Fluid replacement • Antibiotics
Cholecystitis • Most common is a gallstone become lodged in the cystic duct • No known cause of gallstones • Cholecystitis may be related to decreased or absent blood flow
Risk Factors • What is the 4 F’s?
Obesity • Increased Estrogen • Clofibrate • DM • Ileal Disease • Liver disease • Pancreatitis
Disease Process • Similar to Appendicitis • Stone blocks the cystic duct causing a backup of bile & distends the gallbladder (& becomes inflamed) • Bacteria begins to grow (Which one do you think?) • Back up of bile irritates the gallbladder • Cells die in the gallbladder causing increased inflammation resulting in impaired blood flow • Exudate (drainage) occurs
S & S • Usually after a high fat meal • More often at night, may wake a sleeping patient • Pain in the RIGHT UPPER quadrant and radiates to the back, between the shoulders, front of chest • Pain • Belching • Flatulence • Indigestion • Light – headedness • N & V • Chills • Low-grade fever • jaundice
Tests • X – rays – see the stones due to their calcium content • U/S – can confirm as small as 2 mm & see obstructions • Technetium – labeled scan – for difficult to see gallbladders • Percutaneous transhepatic cholangiography – performed with fluoro & looks for obstructions
Treatment • Cholecystectomy • Choledochostomy • Exploration of the common bile duct (surgical) • Endoscopic retrograde cholangiopancreatography • Removes stones with a balloon or basket • Lithotripsy • Crushes gallstones with ultrasonic waves • Low fat diet • Opoids • Antispasmodic & anticholingergics to relax smooth muscles • Anti-emetics • NG tube
Cirrhosis • Chronic Liver Disease • Normal liver cells are destroyed and replaced with fibrous cells • Common cause of death in ages 35-55 • Most common cause?
Portal/nutritional/alcoholic cirrhosis • Caused by alcoholism & malnutrition • Postnecrotic cirrhosis • Complication of viral hepatitis • Exposure of toxins such as arsenic, phosphorus • More common in women • Biliary cirrhosis – prolonged bile duct obstruction • Cardiac cirrhosis – prolonged venous congestion from right sided Heart failure • Idiopathic cirrhosis – No known cause
Effects of Liver malfunction • Blood clotting disorders • Jaundice • Edema • Portal Hypertension • Leads to esophageal varices • Enlarged tortuous veins in esophagus
S & S • Anorexia • Indigestion • N & V • Constipation • Diarrhea • Dull abdominal ache • Jaundice • Easy bruising
Crohn’s Disease • Inflammatory Bowel Disease • Extends through all layers of the intestinal wall & may involve lymph nodes • Ulcers form as the inflammation extends into the peritoneum • Most prevalent 20-40 • Tends to run in families
Progression • Lymph nodes enlarged & lymph flow • Obstruction causes edema, mucosal ulceration, abscesses • Causes thickening of the bowel wall • Became thicker, narrower, & shorter
Treatment • Drug therapy • Corticosteroids • Immunosuppressants • Flagyl • Lifestyle changes • Eliminate fruits, vegetables, & high fiber, dairy, spicy foods, carbonated & caffeinated beverages • Surgery – Colectomy with ileostomy
Diverticular disease • Most common in developed countries • Lifestyle factors contribute to development of disease • Low intake of dietary fiber is a contributing factor • Increased stool bulk decreases the wall tension of the colon • Increased wall tension causes pockets in the colon
Diverticula – bulging pouch in the wall of the mucosal lining • Most common in: • Sigmoid colon • Near the pancreas • jejunum • Diverticulosis – diverticula are present but don’t cause symptoms • Diverticulitis – diverticula are inflamed & can cause potentially fatal obstruction, infection, or hemorrhage
Diverticulitis • Food deposits in the pockets & bacteria begins to grow • Blood can be cut off from the hard food mass • 3 types • Mild – LLQ pain, low grade fever • Severe – Abdomen is rigid • LLQ pain; High fever, chills, hypotension • Chronic – Constipation, intermittent diarrhea, abdomen rigid & pain
Tests • Upper GI series • Barium enema • Biopsy
Treatment • Liquid / bland diet • Mineral oil • Exercise • Antibiotics • Analgesics • Surgery • Colon resection; temporary colostomy
GERD • Commonly known as heartburn • Backflow of gastric or duodenal contents or both into the esophagus & past the cardiac sphincter • Pain may radiate to chest or arms • 36% Americans/ 1/month • Only about 2% with true GERD
Contributing Factors • Weakened sphincter • Increased abdominal pressure • Hiatal hernia • Morphine, valium, Ca+ channel blockers • Alcohol/Smoking
Burning pain • Gastric contents irritate the esophagus • May radiate to arm & chest • Usually after meals or when patient lies down
TESTS • Esophageal acidity test • EGD (what does this stand for?) • Barium swallow • Upper GI series
Treatment • Small meals; do not eat before bed • Sit up during & after meals • Increase fluid intakes • Antacids • Histamine 2 receptors • Proton pump inhibitors • Smoking cessation • Surgery for hiatal hernia
Peptic Ulcers • Lesion in the mucosal membranes • May develop in esophagus, stomach, duodenum, or jejunum • 2 major forms • Duodenal • gastric • 3 major causes • H. pylori (bacteria) causing 90% • NSAIDS • Hypersecrtory states such as Zollinger – Ellison syndrome
Other factors • Blood type A (gastric ulcers); Blood Type O for duodenal ulcers • Genetics • Exposure to irritants • Stress • Aging • trauma
H. pylori • Bacteria that is present in the stomach • Bacteria releases toxin that destroys stomach mucus coat • Reducing the epithelium resistance to acid • Acid burns & causes acid
Tests • EGD • Barium swallow • Upper GI x ray • Stool analysis • WBC count • Gastric secretory studies
Treatment • 1 – 2 weeks of antibiotics • Amoxil • Flagyl • Biaxin • H2 receptor blocker • Tagamet • Pepcid • Proton Pump inhibitor