Download
1 / 16
160 likes | 466 Views
NONOCCUPATIONAL HIV PEP: ACCESS THROUGH HOSPITAL EMERGENCY DEPARTMENTS. John McAllister Clinical Nurse Consultant St. Vincent’s Hospital, Sydney. Hospital emergency departments are key PEP providers. Key component of PEP efficacy is time Key message in the PEP promotion campaign is act fast

E N D
NONOCCUPATIONAL HIV PEP:ACCESS THROUGH HOSPITAL EMERGENCY DEPARTMENTS John McAllister Clinical Nurse Consultant St. Vincent’s Hospital, Sydney
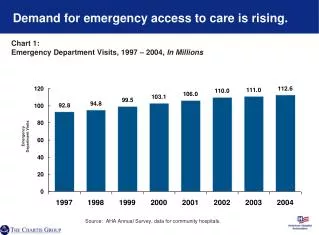
Hospital emergency departments are key PEP providers • Key component of PEP efficacy is time • Key message in the PEP promotion campaign is act fast • Callers to the 1800 PEP NOW service are advised to access PEP immediately • Emergency departments provide a 24-hour service
Hospital emergency departments are key PEP providers • 41.6% (283 of 680) of those enrolled in the National Centre PEP study had their initial PEP assessment through an emergency department • 58% of actual or potential HIV exposures occur on a weekend (St. Vincent’s Hospital Data)
Complete ignorance of PEP there is no such thing Prejudice Privacy Low priority triage 4 or > go see your GP on Monday PEP is an infrequent or rare event in most Eds low presentation rates impede staff familiarisation with the process Poor PEP assessment skills failure to recognise a high risk exposure indiscriminate us of PEP for low/no risk exposures Poor PEP exposure management safety issues inadequate dosing High staff turnover nursing staff junior medical staff Barriers to PEP through an emergency department
Enabling emergency departments to provide quality PEP care • Raise awareness • Provide education • Provide resources and support • Establish a system of data collection & quality monitoring
Raising awareness • Identify key personnel • unit manager • medical director • nurse educator • person responsible for medical intern orientation and education • Words speak louder than circulars
General unit in-service education program Targeted triage nurses the medical staff most likely to be assessing and managing the patient interns Continuous Key components patient privacy & confidentiality sense of urgency triage category 3 risk assessment if in doubt start baseline bloods pre-test counselling the regimen standardised tailored location of the starter packs likely side-effects adjunctive medications 1st dose in ED patient education dosing, side-effects, safety protected sex adherence where to get expert advice/support follow-up & written information Education
Resources & support • Provide a simple risk assessment tool • Provide an algorithm of care • Supplement with a more detailed resource • Make it easy • pre-printed laboratory forms • pre-printed referral slips
CONSIDER PEP IF 1 Unprotected anal or vaginal intercourse Unprotected receptive fellatio with ejaculation Needle sharing 2 Source is known to be HIV infected or belongs to a high risk group 3 The exposure is an isolated event 4 The patient desires and consents to treatment 5 The patient presents within 72 hours 1+2+3+4+5 = PEP
THE PEP PROCESS - INITIAL CONSULTATION • PEP YES • 1st dose of regimen • Supply starter pack • Baseline bloods • Patient education • Provide written material • Supportive counselling Triage 3 PEP NO First Aid Risk assessment Medical History Discuss with HIV consultant on call REFER FOR APPROPRIATE FOLLOW-UP
Establish a system of data collection & quality monitoring • Create a data base • Identify & monitor key markers of quality care • triage scores • length of time between: • triage & assessment • assessment and 1st dose of regimen • Talk to patients, nurses and medical staff • Proactively address issues as they arise • Provide positive feedback
Who is responsible? • HIV Clinical Nurse Consultants • HIV Area Coordinators • own it and implement it
Is it possible?Time in hours from triage to 1st dose PEP - St. Vincent’s Hospital Emergency Department
Development of a state-wide resource for emergency departments and GP’s A Joint project between The Albion Street Centre and St. Vincent's Hospital An HIV/AIDS Health promotion Demonstration Project
Goals to facilitate appropriate access to PEP for all people at risk to ensure appropriate management of community needlestick injuries to reduce the inappropriate use of PEP Objectives ED and GP PEP awareness ED and GP PEP knowledge base PEP quality of care Target group NSW GPs & EDs Strategies evaluate current level of knowledge pre-intervention knowledge surveys design an education resource simple laminated flow chart/algorithm of care education resource pilot resource promote & distribute resource evaluate level of knowledge post-intervention knowledge survey Project: description
Contents: explanation of package flow charts for management reference document with epidemiology and discussion key journal articles NSW Health circulars self assessment tool – case studies and questions Areas to be covered: responsibility risk assessment management referrals For: community NSI sexual exposure skin exposure occupational exposure (less detail) Contents – draft resource