Download
1 / 28
280 likes | 471 Views
Radiation Safety Oversight of Surgical Procedures Involving the Use of RAM. Ren é Michel , M.S., RSO VA San Diego Healthcare System, San Diego, CA. Introduction.

E N D
Radiation Safety Oversight of Surgical Procedures Involving the Use of RAM René Michel, M.S., RSO VA San Diego Healthcare System, San Diego, CA
Introduction The objective of this presentation is to review the various Radiation Safety aspects of a typical medical procedure that involves the use of radiological agents.
Introduction (Cont.) Lymphoscintigraphy (LS) is a medical procedure for the treatment of malignant melanoma and mamma-carcinoma.
Introduction (Cont.) The goal is to identify which sentinel lymph nodes (SLN) have been infiltrated by tumor cells
Introduction (Cont.) The objective of this presentation is to determine what basic radiation safety controls are needed. ALARA, dosimetry, contamination control, radioactive waste, etc.
Outline Radioactive Drugs Used Overview of the Procedure Radiation Exposure Contamination Control Recommendations
Radioactive Drugs Many radiopharmaceuticals have been evaluated for and used in LS studies The ideal drug, must have the following characteristics: Small and uniform particle size Short half-life Low LET Appropriate energy for gamma imaging
Radioactive Drugs 198Au colloid was one of the first widely used drugs in LS 198Au Characteristics Particle size: 3-5 nm Half-life: 2.7 d Emissions: 412 keV photons plus beta particles
Radioactive Drugs 198Au was replaced by other agents with the increased availability of 99mTc Antimony trisulfide, albumin, human serum albumin, sulfur colloid and nano-colloid 99mTc Characteristics Particle size: 3-90,000 nm Half-life: 6 h Emissions: 140 keV photons
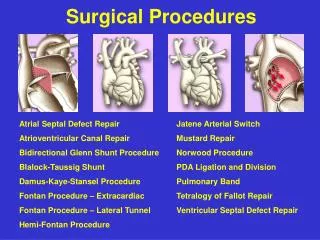
Procedure Overview There are three stages in Sentinel Node LS 1) Lymphatic Mapping 2) Intradermal Blue Dye Injection 3) SLN Biopsy
Lymphatic Mapping The surgeon injects about 1 mCi of 99mTc unfiltered sulfur colloid intradermally near the lesion. The colloid is taken up by the lymphatic system and the patient is imaged with a conventional gamma camera. 2
Lymphatic Mapping (cont.) About 20 min from injection dynamic scanning is performed A late phase scanning done 90 min after injection shows the location of the SLNs. The location of the node is marked on the skin of the patient 2
Blue Dye Injection The patient is moved to the OR to perform biopsy To assist in identifying the nodes draining the site of interest, a blue dye is injected 2
SLN Biopsy A surgeon uses the skin mark and a scintillation probe to relocalize the highest area of uptake
SLN Biopsy (cont.) A dissection is performed through soft tissue to remove “hot” nodes located by the gamma probe All excised nodes are sent to the pathology lab for histological examination to asses for invasion by tumor cells
Radiation Exposure Nuclear Medicine personnel are excluded from this evaluation, they are already closely monitored. 2
Radiation Exposure (cont.) Radiation exposure to OR and Pathology personnel and the potential for spread of contamination are considered the main radiation safety concerns. 2
Hazards Control-Radiation Exposure The expected radiation exposure to personnel from handling SLN radioactive specimens is very small 10-15 SLN procedures/year are performed in most large medical centers Several studies have documented dosimetry data
Hazards Control-Radiation Exposure (cont.) Average whole-body radiation dose equivalent/procedure for hospital personnel from malignant melanoma and mamma-carcinoma SLN surgery with typical activities.
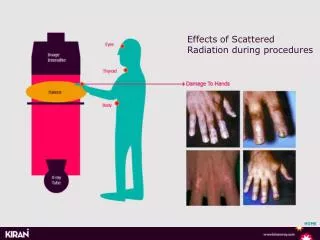
Hazards Control-Radiation Exposure (cont.) A surgeon's hand dose has been reported to be ∽10 mrem (Miner et al. 1999) The pathologist’s hand dose is even smaller, ~ 4-6 mrem (Veronesi et al.1999)
Hazards Control- Contamination The residual activities a day post surgery are <0.3 mCi for tumor-specimens and <50 nCi for SNLE (Kopp and Wengenmair 2002). These activities are relatively fixed to the tissue, they do not produce contamination that exceeds the allowed levels.
Hazards Control- Contamination Standard universal precautions used to prevent infections are sufficient to avoid any kind of incorporation in the bodies of those handling specimens.
Specimen Control Under 10 CFR 20.1905 (NRC 2002), labeling is not required for containers holding less than 1.0 mCi of Tc-99m Labeling is also exempted if only authorized personnel have access to containers, provided a written record identifies the contents. Specimen quarantine before gross examination is unnecessary since the level of exposure to personnel is not a safety concern.
Specimen Control (cont.) Despite the simplicity of the guidelines, each institution is expected to develop and implement procedures for handling radioactive specimens. Awareness training documentation for all individuals handling these specimens is also necessary.
Recommended Guidelines 1. Follow standard universal precautions (e.g., wear hospital gown, surgical gloves, etc.). 2. Using forceps, place all radioactive specimens removed from the patient in a sealed container. 3. In addition to the patient’s name and specimen number, label all resected primary site specimens with the name of the isotope (e.g., 99mTc), date and time when it was collected 4.Maintain security of specimens at all times
Recommended Guidelines 1. Upon completion of the surgical procedure, all instruments (e.g., forceps, scalpels, etc.) having had direct contact with the radioactive specimens should be cleaned following standard procedures. 2. All specimens should follow the normal biomedical waste stream and be surveyed before disposal to ensure that radiation levels are not distinguished from background
References 1. Miner T. et al. Guidelines for the Safe Use of RAM During Localization and Resection of the SLN. Ann Surg Oncol; 6:75-82 (1999) 2. Waddington W. et al. Radiation Safety of the Sentinel Lymph Node Technique in Breast Cancer. Europ J Nuc Med; 27: 377-391 (2000) 3. Kopp, J. and Wengenmair, H. Radiation Protection in Intra- and Post- Operative Diagnosis of the SLN. 6th European ALARA Network Workshop (2002) Tosi, G. et al. Radiation Protection of the Workers in Radioguided Surgery of Breast Cancer. 6th European ALARA Network Workshop (2002) Veronesi U. et al. SLN Biopsy and Auxiliary Dissection in Breast Cancer. J Natl Cancer Inst; 91:368-73 (1999)