Download
1 / 19
251 likes | 488 Views
Human impedance variability and defibrillator test protocol. Why 50 Ω loads are not enough to test modern defibrillators. Defibrillators: life saving. Convert certain heart arrhythmias to normal Convert v-fib back to normal Have to work first time, every time.

E N D
Human impedance variability and defibrillator test protocol Why 50 Ω loads are not enough to test modern defibrillators
Defibrillators: life saving • Convert certain heart arrhythmias to normal • Convert v-fib back to normal • Have to work first time, every time. • Batteries may not be fully charged or faulty • Charging circuits may be faulty, may not deliver enough energy • Must deliver proper energy to account for differing patient sizes/impedances
Current vs. energy • Current—not energy—defibrillates. • Successful defibrillation requires enough current be delivered to the heart muscle during the shock. • Must transit through the chest/thorax and the impedance it represents. • Body mass, skin resistance, tissue type and amount all play a part in the chest/thorax impedance presented to the charge delivered by the defibrillator.
Transthoracic impedance • Transthoracic impedance = the body’s resistance to current flow • Human impedance variability has been shown to vary from 25 ohms to 180 ohms1 • Energy in respect to impedance is the determining factor to successful defibrillation—not energy alone.
Transthoracic impedance (cont.) • Just a few known causes of differing impedances in human beings include: • Body mass • Age • Disease • Skin resistance • Tissue type and amount
Transthoracic impedance (cont.) • Successful defibrillation requires sufficient current to the heart muscle. • Defibrillation current is affected by transthoracic impedance • Modern (biphasic) defibrillators measure impedance and adjust energy delivery accordingly “Humans exhibit a wide range of transthoracic impedance, and defibrillators compensate for this range of impedance in different ways.” -- McDaniel, Garret, Burke and Arzbaecher2
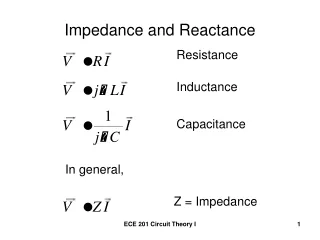
Schematic and formula EH = I2 x RH x Time (Watt Seconds or Joules) Defibrillator
How defibrillators account for human impedance variability • Monophasic (older) defibrillators • Current flows only one direction impedance not measured
How defibrillators account for human impedance variability (cont.) • Biphasic (modern) defibrillators • Current flows first in one direction, then reverses and flows in opposite direction. • Impedance measured and energy delivery is adjusted internally based on energy setting or (for AEDs) arryhthmia.
Biphasic waveforms Q: Are all biphasic waveforms alike? A: No. There are different biphasic waveforms based on different manufacturer’s specifications. Rectilinear Biphasic (ZOLL) Smart Biphasic (Philips) Pulsed Biphasic (Schiller)
Clinical impedance examples • Low impedance (50 Ω) • A 360-joule biphasic defibrillator delivers more current than required, exposing patient to potentially harmful high-peak currents • Average impedance (75 Ω) • A 360-joule biphasic defibrillator and a 200-joule rectilinear defibrillator may be equally effective • High impedance (> 100 Ω) • A 200-joule rectilinear shock delivers a higher average current than a 360-joule biphasic defibrillator shock, therefore making it more effective at lower energy levels.
Impedance and defibrillation outcomes • Too little or too much is no good • Too much peak current during shock can injure the heart • It’s the peak current (not energy) that can injure the heart It is imperative the current delivered to the heart is matched to the individual impedance of each patient and not just the delivered energy.
Load testing: accounting for impedance variability Q: Are 50 Ω test loads enough to ensure output conditions of modern-day defibrillators? • Do all of your hospital’s patients have the same input impedance? No! A: Testing beyond the 50 Ω load is necessary to ensure defibrillator inventory performance of modern defibrillators
Load testing: accounting for impedance variability (cont.) Q: What loads are recommended? A: Section 6.8.3 of the IEC 60601-2-4 standard3 and AAMI DF80 standards4 require defibrillators to be tested on different resistance loads of 25, 50, 75, 100, 125, 150 and 175 ohms to ensure proper current is delivered to patients with different impedances.
When to test with other loads • Each hospital’s equipment history should be considered. • Standard protocol recommends multiple impedance tested on incoming inspection and after a repair to charging circuit or applied parts. • May also be helpful when troubleshooting “failed to deliver energy” complaints.
The 7010 solution • Designed to facilitate load testing for modern defibrillator technology quality assurance and standards compliance • Selectable loads • 25 Ω • 50 Ω • 75 Ω • 100 Ω • 125 Ω • 150 Ω • 175 Ω • 200 Ω • The only device available today capable of testing beyond 175 ohms for extreme impedance conditions. Impulse 7010 Selectable Load Accessory
References • American Heart Association. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Care. Circulation Supplement. 2000; 102:8 • McDaniel W.C., Garrett, M, Burke M.C., Arzbaecher R, Comparison of the Efficacy of Two Biphasic Waveform Defibrillators in a Model of Simulated Higher Impedance Patients, Engineering in Medicine and Biology Soceity, 2003. Proceedings of the 25th Annual International Conference of the IEEE. Volume I, issue 17-21, Sept. 2003 Page(s) 183-185 Vol. I • IEC 60601-2-4 Medical Electrical Equipment Part 2-4: Particular Requirements for the Safety of Cardiac Defibrillators, Section 6.8.3 • ANSI/AAMI DF80:2003 Medical electrical equipment—Part 2-4: Particular Requirements for the Safety of Cardiac Defibrillators (Including Automated External Defibrillators)
References (cont.) Want to know more? Check these out: • Mittal S, Ayati S, Stein KM, Knight BP, Morady F, Schwartzman D, et al. Comparison of a novel rectilinear biphasic waveform with a damped sine wave monophasic waveform for transthoracic ventricular defibrillation. ZOLL Investigators. J Am Coll Cardiol 1999; 34: 1595-601. • Schneider T, Martens PR, Paschen H, Kuisma M, Wolcke B, Gliner BE, et al. Multicenter, randomized, controlled trial of 150-J biphasic shocks compared with 200- to 360-J monophasic shocks in the resuscitation of out-of-hospital cardiac arrest victims. Optimized Response to Cardiac Arrest (ORCA) Investigators. Circulation 2000; 102: 1780-7. • Mittal S, Ayati S, Stein KM, Schwartzman D, Cavlovich D, Tchou PJ, et al. Transthoracic cardioversion of atrial fibrillation: comparison of rectilinear biphasic versus damped sine wave monophasic shocks. Circulation 2000; 101: 1282-7. • Walker RG, Melnick SB, Chapman FW, Walcott GP, Schmitt PW, Ideker RE. Comparison of six clinically used external defibrillators in swine. Resuscitation 2003; 57: 73-83. • Niemann JT, Walker RG, Rosborough JP. Ischemically Induced Ventricular Fibrillation (VF): A Comparison of Fixed and Escalating Energy Defibrillation. Acad Emerg Med 2003; 10: 454.
Questions? For more information on the Impulse 7010 solution for variable impedance testing, contact Fluke Biomedical today. Fluke Biomedical Toll free: (800) 850-4608 Direct: (440) 248-9300 Fax: (440) 349-2307 sales@flukebiomedical.com