Download
1 / 28
280 likes | 447 Views
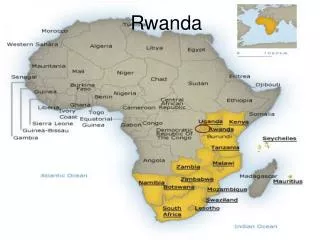
Multi-sectoral Response Rwanda. Anita Asiimwe, MD,MPH Treatment and Research AIDS Centre [TRAC] Rwanda. Rwanda Profile. Genocide in 1994 1 million killed (Former leadership based on exclusion). Current governance structures demonstrated better leadership with principles of equity. 2000.

E N D
Multi-sectoral ResponseRwanda Anita Asiimwe, MD,MPH Treatment and Research AIDS Centre [TRAC] Rwanda
Rwanda Profile Genocide in 1994 1 million killed (Former leadership based on exclusion) Current governance structures demonstrated better leadership with principles of equity 2000 2006 High maternal & infant mortality GDP per capita Primary school enrollment Access to clean water 220 72% 52% 300 92% 70% Illiteracy poverty
Rwanda Profile • Fertility rate: 5.6 • Attend ANC at least once: 90% • Deliveries in health facilities: ~ 30% • Knowledge of individual HIV status among the positives: 42% DHS+ 2005
Strong GOR Coordination • Government Strategy: • CNLS (PMU), PSC, HIV Cluster. • Development Partners: • GOR,USG PEPFAR,GF (3 diseases),WB /MAP,UN-family, ADB, Lux Development • Areas of Coordination: • management, supervision, training, common procurement (drugs, lab equipment, reagents), monitoring and evaluation, performance contracting
Background of MAP Project2003-2007 • project objectives • Strengthen prevention measures to slow down the spread of HIV/AIDS • Expand support and care for those infected or affected by HIV/AIDS Progress was solid with virtually all targets met or surpassed
Established unit within CNLS to manage and coordinate activities (ownership) Harmonized procurement procedures to facilitate joint procurement (economy and alignment) Simplified logical framework (allows poor communities to manage) and synchronized indicators, ensuring consistency in reporting with national M & E plan and national tools e.g TRACnet Program management
Key Components • Health Sector HIV/AIDS Support (US$10.9M): diagnosis, care & treatment • Public Sector Support (US$7.0M): prevention, care & support services • Civil Society Support (US$10.7M.): preventive interventions, OVCs, income-generating activities • Program Management, M & E (US$3.4M.): capacity building, coordination • One Year extension US$ 10M end 2007
care and treatment MAP has financed an expansion in treatment for AIDS patients which has provided life saving ARV therapy to individuals in 14 districts within the context of the national treatment plan
MAP-Supported health facilities offering ARV •Nyagatare
MAP ARV Program • First to extend ART services outside of Kigali, ensuring a pro-poor focus • Developing replicable models of care and support, which are being scaled up with financing from other development partners • Building capacity at sites with no prior experiencethrough facility upgrading, laboratory capacity, HR which in turn has a positive impact on health systems
Schematic of participating health facilities Central oversight and support structures Umutara Provincial and District Health Teams CHK Nyagatare PMU/CNLS TRAC HD HD HD CAMERWA Cyangugu Butare Provincial and District Health Teams Provincial and District Health Teams Gihundwe Butare Univ Hospital HD HD HD HD HD HD CS HF HF HF HF HF
particular results • Majority of patients are poor females who are disproportionately affected by HIV/AIDS • Adherence rate is 96% which is in line with international standards • Patients on 2nd line ARV 1.7% compared to 2.5% national
Résultats cumulés de l'approche contractuelle (fin septembre 06)
Population: Physician Ratio dropped from 45,400 to 34,000:1
High level quality care can be offered in the remotest areas and thanks to HIV and AIDS services that have re-enforced the health system that decentralization supports strongly at the onset Joint planning and field visit including all partners is a way to accelerate harmonization thus supporting to improve care offered Standardizing data collection forms is key to the national program Training & supervising stakeholder in reporting results is key at improving the planning process Decentralize monitoring to district level Ownership of social programs by local authorities Lessons Learned
limited knowledge of planning, management & monitoring of activities & funds for small NGOS insufficient attention to key areas (OVCS, HBC) shortages of personnel, high turnover & lack of incentives time consuming in monitoring and implementation of activities problems to be addressed
conclusion • The philosophy of the MAP project was a very useful innovation for the country and has served as the step stone for the replication of the services country wide. • Strong government coordination in the spirit of the 3 ones, and zero tolerance for corruption has fuelled this success