Download
1 / 33
330 likes | 600 Views
Tissues. -four primary tissue types:. 1. Epithelial. 2. Connective. 3. Muscle. 4. Neural. -however: all tissues in the body develop from three germ layers. 1. ectoderm - epithelial + neural. 2. mesoderm - connective + muscle + some epithelial. 3. endoderm – organs + some epithelial.

E N D
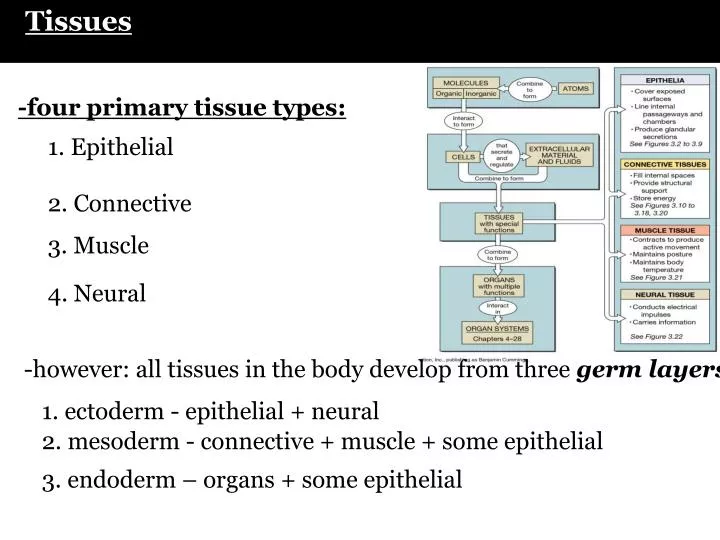
Tissues -four primary tissue types: 1. Epithelial 2. Connective 3. Muscle 4. Neural -however: all tissues in the body develop from three germ layers 1. ectoderm - epithelial + neural 2. mesoderm - connective + muscle + some epithelial 3. endoderm – organs + some epithelial
C H A P T E R F I V E THE SKELETAL SYSTEM: OSSEOUS TISSUE AND SKELETAL STRUCTURE Part A
Skeletal system includes • Bones of the skeleton • Cartilage • Ligaments • Stabilize and connect bones
Functions of Skeletal System • Structural support • framework for attachment • Storage of minerals and lipids • calcium bone salts (1-2 kg: 98% of it in bone) • Blood cell production, triglyceride storage • triglycerides stored in the yellow marrow • RBCs, WBCs, platelets in red bone marrow • Protection of delicate tissues and organs • ribs - heart and lungs; skull - brain; pelvis - digestive and reproductive • Leverage: change the magnitude and forces generated by skeletal muscles
Connective Tissue • binds structures together • provides support • protects organs • fills cavities • produces blood • fills cavities • produces blood • components: matrix + cells -matrix:non-cellular support material -comprised of extracellular protein fibers + ground substance (fluid + sugar) -proteins e.g. collagen fibers, elastic fibers, fibronectin -sugars – e.g. hyaluronan, glucosamine -cells: secrete the matrix -cells vary from tissue to tissue
Connective tissues • Loose – loose/areolar CT, fat & reticular • Dense – dense (regular, irregular), elastic • Supportive – bone & cartilage • Fluid – blood & lymph
Osseous Tissue • Supportive connective tissue • Specialized cells: osteoblasts, osteocytes, OPCs • Solid extracellular matrix • framework of protein fibers: collagen type I • other specialized proteins: osteocalcin, osteonectin, osteopontin • ground substance – sugar + water: e.g. hyaluronan • calcium phosphate crystals: hydroxyapatite
The Histological Organization • Matrix is hydroxyapatite crystals (calcium phosphate) Ca10(PO4)6(OH)2 • as they form - hydroxyapatite incorporates other calcium salts (calcium, carbonate), magnesium, sodium, fluoride • can withstand compression very well • 2/3 weight of bone • remaining 1/3 is collagen fibers, proteins & calcium salts • collagen contributes flexibility • Cells contribute total of 2% total bone tissue volume
Bone formation • also known as osteogenesis • Calcification • Deposition of calcium salts within a tissue • e.g. deposition of hydroxyapatite within bone matrix • matrix calcification = mechanism?? • -controlled by osteocytes • -now known it requires the presence of collagen fibers (framework) • -hydroxyapatite crystallizes in the spaces between collagen fibers • and around the collagen fibers • -may also be controlled by specific bone matrix proteins made • by osteoblasts (e.g. osteocalcin)
Osteocytes • Mature bone cells • maintain and monitor the protein content of bone • completely surrounded by hard bone matrix • directs the release of calcium from bone to blood • directs the deposition of calcium within the bone matrix • do NOT undergo cell division
Osteoblasts • Immature bone-forming cells • cuboidal in shape • found on the inner and outer surfaces of bone • secrete a distinct set of proteins including collagen called the osteoid matrix that will become calcified • non-mineralized matrix = osteoid matrix • collagen I fibers + ground matrix + specialized bone proteins (osteonectin, osteocalcin, osteopontin) • becomes surrounded by a calcifying matrix and then matures to form an osteocyte -do NOT divide
Osteoprogenitor cells • -derived from mesenchymal stem cells (found within the marrow) • -differentiate into immature pre-osteoblasts -> matrix producing osteoblasts -> osteocytes • -undergo division • -play a role in fracture repair
Bone formation 1. formation of OPCs from mesenchymal stem cells within bone marrow 2. differentiation of osteogenic precursors (OPCs) into osteoblasts (OBs) 3. OBs begins to produce the collagenous ECM 4. ECM calcifies into hard bone – formation of HA crystals around the CN fibers 5. OBs mature into osteocytes within lacunae upon this calcification 6. bone maintenance by osteocytes
Osteoclasts (OCs) • large multi-nucleated cells derived from macrophages • attach onto the periosteum or endosteum and move into the bone – carving out tunnels • dissolve bony matrix (osteolysis) through the production of mineral dissolving acids • -also express protein-degrading enzymes called proteases • the components of the digested bone are taken up into the OC and then released into the blood stream • therefore, OC activity can directly regulate calcium and phosphate concentrations in body fluids
Bone Remodelling -so new bone is made by osteoblasts -destruction of old bone during remodelling is by osteoclasts -OCs “carve out” tunnels in the old bone with enzymes and acids – release the calcium and phosphate and amino acids into the blood stream for use elsewhere -OBs enter these tunnels and build up new bone -so there must be balance between new bone production and old bone destruction to maintain bone volume -this balance appears to be controlled by estrogen hormone action in females (increases activity of OBs) -also controlled by the hormones parathyroid hormone (stimulates OCs) and calcitonin(inhibits OCs) -disruption in this balance leads to disease e.g. osteoclast activity exceeds OB - loss of bone = osteoporosis e.g. too high OB activity – bone spurs -high turnover rate – 1/5 of skeleton is remodelled every month -takes 4 months to replace the femur completely -higher level of remodelling in trabecular bone (greater number of OBs and OCs within this type of bone)
Classification of Bones • Based on anatomical classification • Long bones = greater length than width • Short bones = cube-shaped, spongy bone except at surface • Flat bones = two parallel plates of compact bone sandwiching spongy bone layer • Irregular bones = cannot be grouped • Sesamoid bones = develop in tendons where there is considerable friction, tension and stress • Sutural bones = located within joints between cranial bones
Anatomy of Long Bones 1) diaphysis: shaft of the bone 2) epiphysis: distal & proximal ends of bone 3) metaphysis: region where the diaphysis joins the epiphysis -in growing bone it includes the epiphyseal growth plate (hyaline cartilage) 4) articular cartilage: thin layer of hyaline cartilage covering the epiphysis -reduces friction 5) periosteum: dense irregular connective tissue that covers the outside of the bone where not covered with articular cartilage -site of OPCs for bone formation 6) medullary cavity: or marrow cavity -space within diaphysis - contains yellow marrow 7) endosteum: thin membrane that lines the medullary cavity of long bones -single layer of bone forming OPCs
The Periosteum and Endosteum • all bones are covered by periosteum(dense irregular connective tissue) • Outer fibrous layer • Inner cellular layer (osteo-progenitor cells) • Long bones are also lined by endosteum which also contains progenitor cells + numerous osteoclasts
Compact and Spongy Bone • matrix of bone can be described as one of two patterns: • 1) compact bone • 2) spongy bone 1) Compact = dense bone -contains few spaces -makes up the bulk of the diaphysis - also forms the outer layer of short, flat and irregular bones -arranged in units called osteonsor Haversian systems -osteons run the length of the bone’s shaft
connects with those vessels & nerves in the Central canals or Haversian canals (longitudinal orientation) • around these canals are concentric • circles of bone = concentric lamellae Osteon or Haversian System • blood vessels, lymphatic vessels and nerves from the medullary cavity and periosteum penetrate the bone through perforating canals or Volkaman’s canals (transverse orientation
Osteon or Haversian System • between the lamallae are • small spaces in the matrix containing cells = • lacunae • the lacunae are connected • by canaliculi filled with • extracellular fluid and cellular • projections from the osteocytes • the canaliculi connect every lacunae • to the central canal • areas between osteons are filled • with interstitial lamellae that also • have lacunae and canaliculi - are • fragments of older osteons that • are being degraded • osteons are aligned along the • bone in the same direction as • stress • e.g. shaft - parallel to the long axis
Bone histology • this is what calcified compact bone looks like under the microscope
Spongy Bone • 2) Spongy bone • -same matrix as compact bone • -different arrangement of osteocytes, canaliculi and lamellae • -does not contain osteons • -consists of trabeculae = irregular lattice of thin bone columns • -spaces between trabeculae are filled with red marrow • -the trabeculae are arranged along lines of stress - resistance to breakage
-the trabeculae also have lamellae with lacunae containing osteocytes -spongy bone makes up the majority of the irregular, flat and short bones of the body e.g. hip, ribs, sternum, ends of long bones (femur) -often covered by a thin layer of compact bone -because of presence of red marrow - spongy bone is the site of hematopoiesis in adults (blood cell formation)
Spongy vs. Compact Bone • Spongy bone is lighter - reduces overall weight of the bone • Spongy bone contains red marrow - vs. the yellow marrow found in the medullary cavity surrounded by compact bone
Circulatory Supply to a Mature Bone -bone has a rich blood supply -blood vessels are abundant in bone portions containing red marrow -periosteal arteries + nerves enter the diaphysis through the perforating/Volkmann’s canals -they supply the outer periosteum and the outer part of the compact bone -a large nutrient artery enters the medullary cavity around the center of the bone shat through a hole in the compact bone = nutrient foramen
lymphatic vessels enter osteons through perforating canals and nutrient vessels • Sensory nerve endings branch throughout periosteum • Sensory nerves enter center of bone with nutrient vessels
Injury and Repair • Fracture is a crack or break in a bone • Healing occurs if portions of periosteum, endosteum and blood supply remain
infiltration of blood vessels organizes the hematoma into a procallus, fibroblasts and stem cells from periosteum, endosteum and marrow invade and make new matrix at bone ends, chondroblasts also produce a fibrocartilage callus fragments of broken bone are resorbed by OCs, compact bone replaces the spongy bone of the callus • Steps involved in the repair of a fracture. bony callus lasts 3 to 4 months circulation stops in this region and OBs die immune cells arrive + OCs - damaged tissue removed
Clinical Discussion – A Classification of Fractures -open fracture: broken ends protrude through skin -comminuated fracture: bone splinters at site of impact -Greenstick fracture: partial fracture - one side breaks, the other side bends -impacted fracture: one end is driven into the interior of the other -Pott’s fracture: fracture at distal end of fibula -Colles’ fracture: fracture at distal ends of forearm bones - distal fragment is displaced posteriorly