Download

1 / 66
670 likes | 965 Views
Genetics and Cancer. Sreekala Seepana. Overview. Genetics and cancer Breast / Bowel cancers Breast / bowel cancer screening Clinical genetics referral Cases Others. What’s my risk, doc??.

E N D
Genetics and Cancer Sreekala Seepana
Overview • Genetics and cancer • Breast / Bowel cancers • Breast / bowel cancer screening • Clinical genetics referral • Cases • Others
What’s my risk, doc?? • People whose relatives have cancer or have died of cancer may be worried that they too could develop cancer • Patients who have cancer themselves may be concerned about whether other members of their family might be at risk • Patients who are enrolled in programmes for cancer screening may become aware that their family history may predispose them to developing cancer
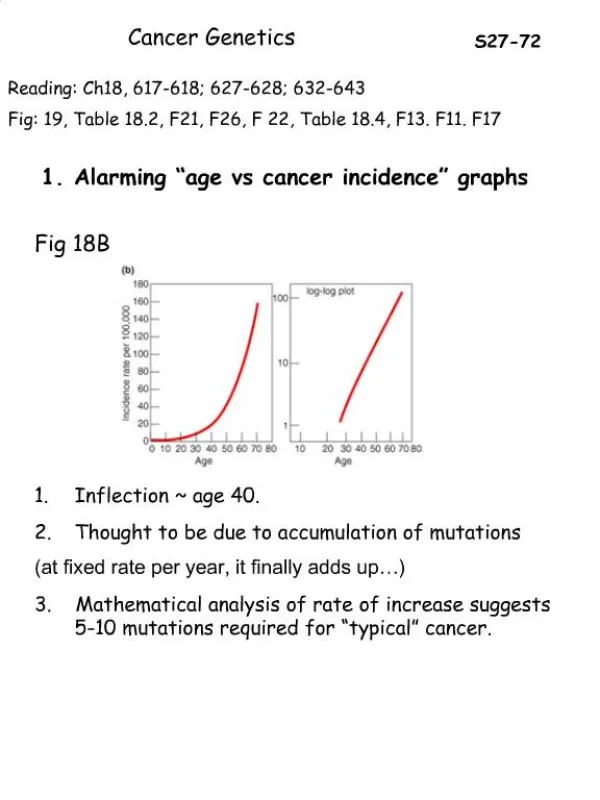
Genetics and cancer • 5-10% of cancers due to genetic factors • Cancer genes greatly increase the risk of a person developing cancer • Genes that predispose to cancer are not in X or Y chromosome • Family history is the most reliable way of assessing the familial risk of developing cancer • Refer pts identified at high risk of developing cancer for screening and specialist assessment of family history
Genetics and Cancer • Family history is vital • Explore family history of 3 generations • Family history should include those affected and those unaffected by cancer • Specific type of cancer • Age at which cancer developed Clues to familial cancers.....?
Familial cancers Clues: • Two or more close relatives with same type of cancer • Cancer at early age (usually < 40yrs) • Cancer diagnosed more than once in the same person • Many cancers in the family, not accounted for just by chance • Cancer in a person who also has some birth defects Breast cancer /ovarian cancer Colorectal cancer Renal cell carcinoma (Von HippelLindau disease ) Wilms tumour Li Fraumeni syndrome (TP 53) Retinoblastoma, osteosarcoma
Family history of cancer All relatives must be on the same side of the family and blood relatives of the consultee and of each other • First degree relatives: mother, father, daughter, son, sister, brother. • Second degree relatives: grandparent, grandchild, aunt, uncle, niece, nephew, half sister, and half brother. • Third degree relatives: first cousins.
Cancer genes • Mutations occur in normal functioning genes • Risk of cancer that these genes confer is organ specific • People with mutated genes have an increased risk of developing cancer, but some may never develop cancer
Types of genes which may mutate to cause cancer • Tumour suppressor genes • oncogenes • DNA repair genes • telomerase • Tp 53
Estimated risk of developing breast cancer by age, females, UK, 2001–2005 Cancer Research UK
Risk factors for breast cancer • Female sex • Increasing age • Previous h/o breast ca • Benign breast disease • Not breast feeding long term • Current use of HRT /COCP • Nulliparity • Late pregnancy • Early puberty • Late menopause • Obesity • High alcohol intake • Family h/o breast cancer
Important messages to share with women with concerns • Most of breast cancers are not familial • Increasing age is the greatest risk factor • The great majority of women with a family history of breast cancer do not fall into a high risk category and do not develop breast cancer • The great majority of women with a relative with breast cancer are not at substantially increased risk of breast cancer themselves NICE 2006
Breast cancer “Why do so many of my relatives have breast cancer...is this just plain bad luck or what?”
BRCA 1 and 2 • BRCA1 on 17(q) • BRCA 2 on 13 (q) • High penetrance genes, responsible for < 10% of breast cancers • Called “breast cancer genes” but increase the risk of breast and ovarian ca. • Life time risk of developing breast ca of up to 85% (UK population risk of 11%) and ovarian cancer of up to 60% (UK population risk of <2%)
Familial breast cancer BRCA 1 BRCA 2 Causes 40% of familial breast cancers 50-70% - breast cancer 15-45% - ovarian cancer Increased risk of prostate and colon cancers • 50-70% - breast cancer • 20-30% - ovarian cancer • Increased risk of prostate, laryngeal, pancreatic cancers
Rare familial cancer syndromes associated with breast cancer: Cancer Research UK
Which one of the following population groups have the highest incidence of having BRCA 1 & 2 : • English • Scottish • Asian • Chinese • Jewish • Polish
Which one of the following population groups have the highest incidence of having BRCA 1 & 2 : • English • Scottish • Asian • Chinese • Jewish • Polish Women with Jewish ancestry have about 5-10 times more likely to carry BRCA 1 &2 mutations
Relative risk for breast cancer by number of affected first degree female relatives Risk of familial breast ca is quantified with respect to the number of affected first degree relatives and by the age of affected first degree relative
Relative risk for breast cancer by age of affected first degree relative
Risk categorization (NICE) • Near population risk: • women at or near population risk of developing breast cancer (that is, a 10-year risk of less than 3% between age 40 and 50 years and a lifetime risk of less than 17%) are cared for in primary care • Raised risk: • Women at raised risk of developing breast cancer (that is, a risk of 3-8% between age 40 and 50 years or a lifetime risk of 17% or greater but less than 30%) are generally cared for in secondary care • High risk: • Women at high risk of developing breast cancer (that is a risk of greater than 8% between age 40 and 50 years or a lifetime risk of 30% or greater) are cared for in tertiary care. High risk also includes a 20% or greater chance of a faulty BRCA1, BRCA2 or TP53 gene in the family
Referral to secondary care(likely to be at more than raised risk) Female breast cancers only: • One 1st degree relative and one 2nd degree relative diagnosed before average age 50 • Two 1st degree relatives diagnosed before average age 50 • Three or more 1st or 2nd degree relatives diagnosed at any age
Referral to secondary care(likely to be at more than raised risk) Bilateral breast cancer • One 1st degree relative where 1st primary diagnosed before age 50 • For bilateral breast cancer, each breast has the same count value as one relative Male breast cancer • One 1st degree male relative diagnosed at any age
Referral to secondary care(likely to be at more than raised risk) Breast and ovarian cancer • One 1st or 2nd degree relative with ovarian cancer at any age and one 1st or 2nd degree relative with breast cancer at any age (one should be a 1st degree relative)
Referral to secondary care Likely to be at raised risk: (Female breast cancers only) • One 1st degree relative diagnosed before age 40 • One 1st degree relative and one 2nd degree relative diagnosed after average age 50 • Two 1st degree relatives diagnosed after average age 50
Surveillance • All women aged 40–49 years satisfying referral criteria to secondary or specialist care (at raised risk or greater) should be offered annual mammographic surveillance.
MRI surveillance • Women who are known to have a genetic mutation should be offered annual MRI surveillance if they are: – BRCA1 and BRCA2 mutation carriers aged 30–49 years – TP53 mutation carriers aged 20 years or older.
MRI surveillance MRI surveillance should be offered annually when indicated: From 30–39 years: • to women at a 10-year risk of greater than 8% From 40–49 years: • to women at a 10-year risk of greater than 20%, or • to women at a 10-year risk of greater than 12% where mammography has shown a dense breast pattern
Role of prophylactic surgery Prophylactic mastectomy in women at high genetic risk of developing breast cancer reduces the risk of breast cancer by up to 90%
Percentage distribution of cases by site within the large bowel, England, 1997-2000
Familial bowel cancers • Familial adenomatous polyposis (FAP) • Heriditary non-polyposis colorectal cancer (HNPCC) or Lynch syndrome • Rare polyposis - Peutz-Jeghers syndrome and familial juvenile polyposis (autosomal dominant)
Familial adenomatouspolyposis • Gene for FAP is the APC (adenomatous polyposis coli) tumour suppressor gene on 5q21
Familial adenomatouspolyposis • Accounts for 1% of colorectal cancers • Multiple (often thousands) of adenomas in large bowel • Almost 100% risk of developing colorectal cancer by 40yr • Prophylactic surgery is offered to affected individuals, usually in their teens.
HNPCC (Lynch syndrome) • Accounts for 2-5% of colorectal cancers • Caused by fault in a DNA mismatch repair gene (MMR gene) MLH1 and MSH2 genes • Characterized by early onset of bowel cancer
HNPCC (Lynch syndrome) Associated with non-colorectal cancers: • endometrium, • ovaries, • stomach, • pancreas / liver • urinary tract
HNPCC (Lynch syndrome) • Genetic testing for predisposing mutations in people with a strong family history of these cancers enables screening and prevention to be targeted to those most at risk. • For people with a known mutation, especially young patients from HNPCC families, prophylactic surgery may be recommended
Which of the following patients are offered NHS breast cancer screening: a. Every 2 yrs for women aged 50-70yrs b. Every 2 yrs for women aged 60-70yrs c. Every 3yrs for women aged 60-70yrs d. Every 2.5yrs for women aged 50-70yrs e. Every 3 yrs for women aged 50-70yr
Which of the following patients are offered NHS breast cancer screening: a. Every 2 yrs for women aged 50-70yrs b. Every 2 yrs for women aged 60-70yrs c. Every 3yrs for women aged 60-70yrs d. Every 2.5yrs for women aged 50-70yrs e. Every 3 yrs for women aged 50-70yr
Figure One:Number of new cases and rates for female breast cancer, by age, UK, 2006 Cancer research ,UK
Breast cancer screening • Aim is to detect early, non-palpable, local disease. • Mammographic screening – reduced mortality rate of at least 25% in women over the age of 50. • After 10 years, the UK screening programme is expected to produce a reduction of 1250 breast cancer deaths annually, with each woman in whom death from breast cancer is prevented, surviving, on average, an extra 20 years.
Breast cancer screening programme The main elements are: • to invite three-yearly, all women in the 50-70 year age group for single oblique-view mammography in static or mobile units, with the option of self-referral for older women • to recall all women with mammographically detected abnormalities for further investigation in specialist assessment units, using clinical examination, special view mammography, ultrasonography, or fine needle aspiration cytology
UK NHS Breast Screening Programme results April 2006 to March 2007 Cancer research UK
NHS breast screening programme • Women are invited to a specialised screening unit, which can be hospital based, mobile, or permanently based in another convenient location such as a shopping centre.
NHS breast cancer screening programme in Grimsby is based in : • X-ray unit in Radiology dept, DPoW • MRI unit in Radiology dept, DPoW • CT unit in Radiology dept, DPoW • Breast clinic, DPoW • Opposite to Canteen, DPoW • Car park opposite to library, DPoW
NHS breast cancer screening programme in Grimsby is based in : • X-ray unit in Radiology dept, DPoW • MRI unit in Radiology dept, DPoW • CT unit in Radiology dept, DPoW • Breast clinic, DPoW • Opposite to Canteen, DPoW • Car park opposite to library, DPoW