Download
1 / 22
240 likes | 361 Views
Cancer Genetics. Issues. Colorectal guidelines Awaiting publication of coloproctologists guidance SIGN / QIS update started Breast / ovarian Breast MRI Minor changes to guidelines? NF1 Average age v absolute ages Incorporate pathology into testing criteria? Change to English guidance?

E N D
Issues • Colorectal guidelines • Awaiting publication of coloproctologists guidance • SIGN / QIS update started • Breast / ovarian • Breast MRI • Minor changes to guidelines? • NF1 • Average age v absolute ages • Incorporate pathology into testing criteria? • Change to English guidance? • Trials to report – UKFOCSS, FH01 etc • Other conditions – gastric, renal etc.?
Breast cancer • Breast MRI • NF1 • English guidelines? • FH01 study results – confirm effectiveness, reduce mortality • Molecular testing • Triple negative young women (<30) • High grade serous ovarian cancer? • BRCA3 results by Manchester score • Double primary breast and ovary - audit
Proposals from last meeting • Modify mutation testing to allow pathology data to be used where available • Test ovarian cancers with visceral metastases?, or all high grade serous ovarian cancers • Meeting of small group with Dr Gourlay • Aberdeen d/w NSD funding additional testing • Glasgow propose trainee project to assess yield • Lower threshold if impacts management (PARPi) – BRCA3 info
Ovarian BRCAness meeeting • Should we test more women with ovarian cancer? • Visceral mets, young age, response to platinum, prolonged survival • High grade serous • Literature – no ideal series. One publication suggests 23% of high grade serous have BRCA1 mutation but ascertainment / possible founders etc not clarified. • Agreed helpful to have further information in our population group. ?test for 12 months and look at data. • Oncologists also interested in somatic mutations • Not currently influencing treatment but will in future
Ovarian BRCAness meeeting • Practicalities • Need family history and pathology info • Consent issues • Suggest take blood at initial meeting, store until consent sorted out. • Joint leaflet for patients, standard request / consent form / referral form. Refer if positive? • ?additional capacity Aberdeen • Numbers – 350 high grade serous / year? • Oncology meeting in November • Audit previous ovarian testing? (? Info to CG)
Ovarian BRCAness meeeting • Technical issues • ?tumour testing • ? Rebiopsy to look for second mutations, mets etc • ?other pretest would be useful? RT-PCR, antibody stains etc??
Ovarian cancer in Glasgow • Robots in molecular lab, improved turnaround for BRCA2 dramatically. • Previously reluctant to consider ovarian samples, now willing to consider a trainee project • Store blood from ovarian cancer patients • If high grade serous / FH / long survival etc, refer to genetics to consider testing
UKFOCSS • No longer recruiting • Scans will end 2011 • No plans to arrange any ongoing screening, will leave to gynaecologist • UCL suggest baseline investigations at first appointment, discuss surgery etc
BRCA3 results by Manchester score • 618 results. Scores 4-65. 56 mutations (9%), 31 BRCA1, 25 BRCA2. • 18 mutations in 446 with score <20. (4%). 3 with ovarian FH, of 33 with ovarian history. • 38 mutations in 172 with score >20. (22%) • Score of 16+: 47 mutations in 290 (16%) [4%] • Score of 18+: 44 mutations in 221 (19.9%) [8%]
Double Primary breast / ovary • Breast / ovary double primaries • 57 tested. 54 full results • 17 BRCA1, 9 BRCA2, 6 VUS found. 46% pickup. • Manchester score over 20 – 66% pickup (22/33) • Manchester score <20 – 36% detection (4/11)
Triple negatives / young br ca • Little data yet! 16 samples tested which say triple neg on database. 7 BRCA1 mutations, 2 BRCA2, 2 VUS. (56%) • Breast cancer under 30: 18 samples tested, 5 BRCA1, 2 BRCA2, 1 VUS BRCA2. (44%) • Additional 4 <30 with p53: bilat breast ca under 30, br ca 29 with affected M and MA, br ca 29 with relative CACC, br ca 29 with osteosarcoma.
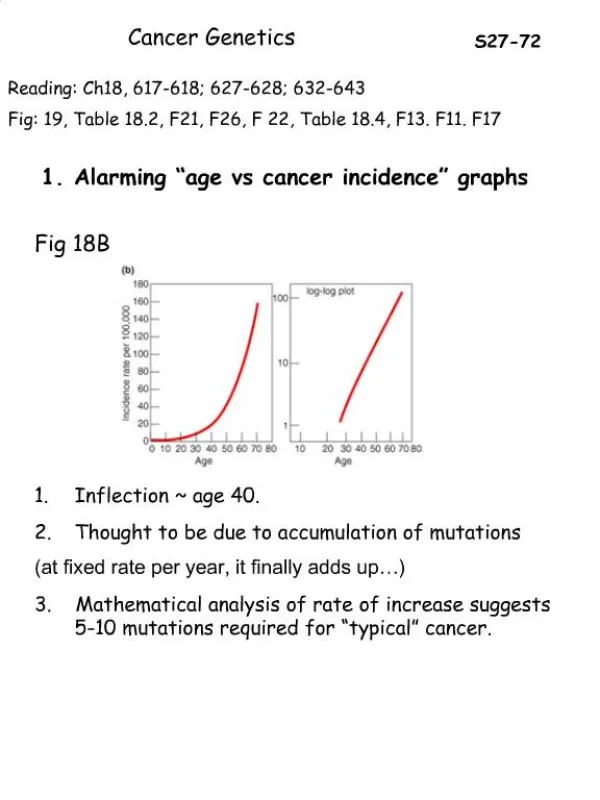
FH01 study • 6710 women under 50 at moderately increased risk, control group from age trial and Dutch series. FU 5 years, annual mammo. • 136 breast cancers diagnosed, 77% screen detected, 21% interval cancers. Tumours smaller, less likely node positive, moe fabourable grade. • Predicted mortality significantly lower. (Prevent 2.1 breast cancer deaths per 10,000 screens.)
IMPACT study • Ready to recruit in Glasgow • 4 men agreed to take part, 17 BRCA2 positive and 12 BRCA2 negative eligible. • Not yet approached BRCA1 men.
Lower testing threshold? • When management shown to be impacted • Contralateral mastectomy • PARP inhibitor trial results
England • NICE guidance 2004 / 2006 • 1 under 40, 2 first degree relatives any age • Risk 1.7x population risk, 3% 10 year risk at 40 • Now looking again at this, want to look at survival benefit. • Proposal to look at women with 4x risk, 18 monthly mammography from 40 to 73. No screening for those at lesser degrees of risk.
Molecular testing • Young women with triple negative tumours? • Management impact? • PARP inhibitor trials • Contralateral mastectomy • Recent paper looking at large series with breast cancer and BRCA testing, by age and BRCA status • Changed 10 year risk from 6% to 28% • Incorporation of pathology data – • Manchester score: simple to use • BOADICEA: complicated to use
BRCA1 • More likely ER-, HER2- • Less likely grade 1 • -4 for HER2+. +4 for grade 3 triple negative • Overall sensitivity and specificity increased • Suggest testing women <31 with triple negative disease for BRCA1, no other groups over 10% threshold without family history
Contralateral mastectomy • Series of 705 bilateral cases and 1398 unilateral controls, from cancer registry in US, cohort of 52000 diagnosed under 55 • BRCA testing • 5 and 10 year risks of contralateral breast ca by age of first diagnosis • 28% v 6% at 25-29 y • 19% v 4% at 40-44y • 10% v 4% at 50-54y