Download
1 / 34
340 likes | 521 Views
Endocrine Board Review. Growth. Growth can be easiest way to determine overall health of a child Red Flag: Growth less than 5 cm/year Most common cause of short stature is short parents. Growth Hormone. Secreted in response to GHRH Is secreted in bursts Dopamine causes release of GHRH

E N D
Growth • Growth can be easiest way to determine overall health of a child • Red Flag: Growth less than 5 cm/year • Most common cause of short stature is short parents
Growth Hormone • Secreted in response to GHRH • Is secreted in bursts • Dopamine causes release of GHRH • Somatostatin inhibits the release of GH • Anything that effects the pituitary gland will usually result in GH Def. • Think midline defects, central incision, bifid uvula
Growth Hormone Deficiency • Height less than 3 SD below mean, slow growth velocity • Characteristic Features • Short stature • Normal body proportion • Increased adiposity around trunk and extremities • Boys may have small genitalia • Can be seen with midline defects • Hypoglycemia
Growth Hormone Def • Tests • Height and bone age is delayed • Low IGF-1 and low GH levels • Can do GH stimulation tests • Exercise • L-Dopa, insulin, arginine, clonidine, glucagon • Treatment • GH replacement
THINK Hypopituitary • Hypoglycemia • Micropenis • Jaundice • Midline facial abnromalities
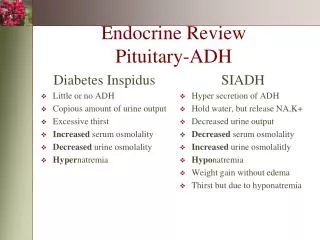
Thyroid Hormone • TRH TSH T4/T3 • Free T4 is the only active form
Congenital Hypothyroid • Most are asymptomatic at birth because of maternal thyroxine • Newborn screen will check TSH • Clinical Presentation • Infant can present with goiter • Broad nasal bridge, thick lips, poor feeding • “hoarse cry” • Slow heart rate, low temperature • Umbilical hernia • Large posterior fontenelle, large sutures on X-ray
Congenital Hypothyroidism • Most common cause is thyroid dysgenesis • Other less common causes • Defect in the synthesis • Radioiodine given during pregnancy • TSH deficiency • Treatment should be started within 2 weeks • Thyroxine • Good prognosis if started early in life
Acquired Hypothyroid • Most common cause Hashimoto thyroiditis • Dry skin, constipation, hair loss, depressed DTR, goiter • More common in girls • Sharp deceleration of growth with preserved • Tests • High TSH • Low thyroxine level • Often detect antibodies SCFE – high risk with rapid changes of growth. Can see because of rapid halt!
Hyperthyroid • Graves disease is most common cause • TSH receptor antibody stimulates thyroid cells • Symptoms • Tachycardia, weight loss, heat intolerance • Anxiety, muscle weakness, tremor • Exophthalmos,Goiter • Tests • Elevated thyroxine and triiodothyronine • Low TSH • Treatment • PTU or methimazole • Surgery – radioactive iodine/thyriodectomy
Turner Syndrome • Common cause of short stature in girls • Physical findings • Cubitusvalgus, sheildlike chest, web neck • Gonadal failure • Pubic and axillary hair with no breast development or menarche • WorkUp • Karyotype
The PARATHYROID???? • PTH • Increased Ca+ release from bones • Decrease renal excretion of Ca+ • Increase conversion of Vit D to 1,25 OH-D • Decreases Phosreabsorption from kidney • 1,25 OH-D • Increase Ca+ reabsorption from gut, bone, kidney • Increase phosreabsorption from gut and kidney
Calcitonin • “PTH antagonist” • Decrease Ca+ bone resorption • Increases renal Calcium clearance
Hypoparathyroidism • Due to aplasia/hypoplasia of parathyroid gland • Can be associated with DiGeorge • Also autoimmune forms • Presentation can vary • Muscle pain or cramps • Positive Chvostek or Trousseau sign • Seizures
Hypoparathyroidism • Labs: • Hypocalcemia • Elevated phos • Low PTH/low 1,25 OH D • EKG: prolonged QT • Treatment • Calcium • Vit D (Calcitriol)
Albright Hereditary Osteodystrophy • Pseudohypoparathyroidism • Round facies, short stature, obesity, skin hyperpigmentation, short thick necks • Short 4th metacarpals and metatarsals • Decreased intelligence • Labs • Hypocalcemia • Hyperphosphatemia • Elevated PTH
Hyperparathyroid • In children usually response to low Ca+ levels • Vit D deficiency • Malabsorption • Chronic renal disease • MEN I – neoplasia • Pancrease • Parathyroid • Pituitary
Cushing Syndrome • Excess glucocorticoid secretion • Clinical features • Round face, obesity, buffalo hump, stirae, thin extremities, HTN, osteoporosis, decrease growth, hirsutism • Testing • Elevated urine free cortisol • Dexamethasone suppression test • Causes • Adrenal tumor, pituitary adenoma, ectopic ACTH
Cushing Disease • ACTH-secreting pituitary tumor • Which results in excess glucocoriticoid secretion
Addison Disease • Acquired Deficiency of glucocorticoid and mineralcorticoid • Clinical Features • Thin body, hyperpigmentation of skin(bronzing) • Confusion, weakness • Can cause vascular colapse • Testing • Hyponatremia, hyperkalemia, low cortisol • Treatment • Replacement of hormones
Congenital Adrenal Hyperplasia • Autosomal recessive • Get increased ACTH • Causes: • 21-Hydroxylase Def • Most common cause • Salt wasting • Virilization • Elevation 17-Hydroxyprogesterone • 11ß-Hyroxylase Def • No salt wasting – hypertension • Virilization • Elevated 11-deoxycortisol
Congenital Adrenal Hyperplasia • Presentation • Shock or septic in newborn • FTT • Males – normal genitalia (could have hyperpigmentation of scrotum) • Females- ambiguous genitalia • Lab findings • Low Na • Low Cl • High K