Download
1 / 27
280 likes | 747 Views
Chapter 13: Brainstem and Basal Ganglia. Chris Rorden University of South Carolina Norman J. Arnold School of Public Health Department of Communication Sciences and Disorders University of South Carolina. Afferent Fibers. Spinal Ganglia. Muscle. Efferent Fibers. Dermatomes.

E N D
Chapter 13: Brainstem and Basal Ganglia • Chris Rorden University of South Carolina Norman J. Arnold School of Public Health Department of Communication Sciences and Disorders University of South Carolina
Afferent Fibers Spinal Ganglia Muscle Efferent Fibers
Dermatomes Branches of Cranial Nerve V (Trigeminal) Opthalmic Maxillary Mandibular
Chickenpox Shingles
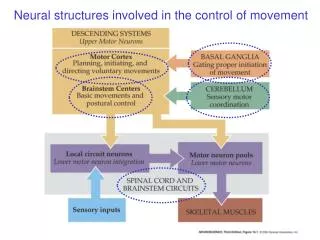
Brainstem Motor Mechanism • Motor • Pyramidal • Corticospinal tract and corticobulbar tract • Extrapyramidal • Facilitatory, inhibitory, and/or regulatory • Red Nucleus • Part of midbrain • Cranial Nerve Nuclei • Reticular Formation
Brainstem Anatomy • Red Nucleus • Rubrocerebellar Tract • Important for gait in animals without significant corticospinal tract • Humans: upper arm and shoulder • Cranial Nerve Nuclei • Will Be Discussed With Cranial Nerves • Reticular Formation • Focus in This Chapter
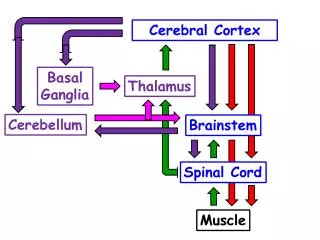
Reticular Formation • Located between caudal diencephalon & spinal cord • Network of Overlapping Dendrites and Axons • Input From • Motor Cortex • Basal Ganglia • Cerebellum • Cranial Motor Neurons
Reticular Formation Function • Arousal • Tonal Modulation • Pain Processing • Regulation of • Vomiting • Coughing • Cardiovascular Functions • Respiration • Speech Functions
Reticular Nuclei • Reticularis Gigantocellular • Pontis Oralis and Cudalis • Lateral Reticular Nucleus • Ventral Reticular Nucleus • Paramedial Reticular Nucleus • Interstitial • Raphe • Ceruleus
Reticular Motor Functions (1) • Examined in anencephalic children who have no cortex or cerebellum • Muscle Tone Regulation - Maintains Balance of Stimulation
Reticular Motor Functions (2) • Facilitatory Reticular Areas • Upper and Lateral Brainstem • Increases Muscle Tone in Extremities • Sleep wake cycle, alertness • Inhibitory Reticular Areas • Lower and Medial Region of Medulla • Decreases Muscle Tone in Extremities • Posture, equilibrium, motor control ascending reticular formation descending reticular formation
Clinical considerations • Disconnection of cortex and basal ganglia from reticular formation • Decerebrate Rigidity • Extensor posturing of all Limbs • Excessive facilitatory impulses • Transection Below Vestibular Nucleus • Flaccid Paralysis • Similar to degeneration of the lower neuron
Basal Ganglia • Modify cortically initiated motor movements (speech) • Caudate Nucleus • Putamen • Globus Pallidus • Related Brainstem Structures • Substantia Nigra • Subthalamic Nucleus
Results of Basal Ganglia Impairment • Involuntary Motor Movements • Bradykinesia (slow) or Hypokinesia (slow or diminished) • Altered Posture • Changes in Muscle Tone • Implicate Neurotransmitters • All Result in Dysarthria and Dysphagia • Parkinson’s Disease • Huntington’s Disease
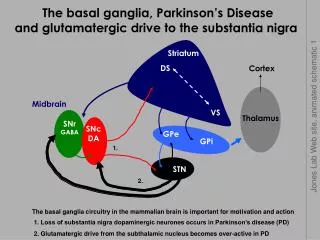
Basal Ganglia • rostral • striatum • putamen • caudate nucleus • nucleus accumbens • globus pallidus • caudal • subthalamic nucleus (STN) • substantia nigra (SN)
Aliases • Lenticular Nucleus • Putamen and Globus Pallidus • Neostriatum or Striatum • Caudate Nucleus and Putamen • Pallidum • Globus Pallidus
Structures • Caudate Nucleus • Elongated C Shaped Mass With Head and Tail • Bordered by Ventricles, Internal Capsule and Temporal Lobe • Globus Pallidus Next to Putamen • Putamen Connected to Head of Caudate Nucleus
Neurotransmitters • Dopamine • Inhibitory Neurotransmitter • Produced in the substantia nigra and secreted in the striatum • Acetylcholine • Facilitatory/Inhibitory Neurotransmitter • Gamma-Aminobutyric Acid • GABA Regulates Adjacent Structures • e.g. thalamus
Clinical Considerations • Athetosis • Involuntary slow writhing (twisting) movement • Continuous stream of slow, sinuous, writhing movements, typically of the hands and feet. • Varying degrees of hypertonia • Usually seen in lesions of the globus pallidus • Ballism (Subthalamic Nuclei – Diencephalon, chapter 6) • Violent Forceful Flinging of Arms and Legs • Most violent form of dyskinesia (movement disorder) • Usually associated with lesions in the sub-thalamic nucleus (which regulates the globus pallidus) • Hemiballism: unilateral ballism (e.g. unilateral stroke) • Can be treated with dopamine blockade or resection of GP.
Clinical Considerations • Chorea • Series of rhythmic involuntary movements • Predominantly in the distal extremities and muscles of the face, tongue, and pharynx • Chorea is characterized by brief, irregular contractions that are not repetitive or rhythmic, but appear to flow from one muscle to the next. • These 'dance-like' movements of chorea (from the same root word as "choreography") • often occur with athetosis and more severe cases present with ballism
Forms of Chorea • Sydenham’s Chorea (rheumatic fever 5-15 years old) • Secondary to streptococcal infection • Most recover completely (with problems for a few months) • Huntington’s Chorea (aka Huntington’s Disease) • 1872, George Huntington • Treated families with same characteristics • Heredity, Adult Onset, Chorea, Cognitive Loss • Autosomal Dominant • 5 in 100,000 prevalence • Equal in Men and Women • Loss of Cholinergic and GABAnergic neurons in Caudate Nucleus
Autosomal Dominant Traits • the trait, half the children will have the trait. • Example: being a boy. Your father has one copy of the Y chromosome, and one X. Each child has a 50% chance of being a boy.
Clinical Considerations • Dyskinesia • Generalized Disorder of Involuntary and Voluntary Movement • Masked Face, Infrequent Blinking, Slow Movement, Disturbed Equilibrium, Stooped Posture, Impaired Speech, Impaired Swallowing • Tremors • Alternating Movement of Opposing Muscles • Resting Tremor
Basal Ganglia Diseases • Parkinson’s Disease (1817, James Parkinson) • Tremor at Rest • Cogwheel Muscular Rigidity • Bradykinesia (Slow execution of body movements) • Akinesia (Slow beginning or inability to initiate a movement) • Shuffling Gate • Expressionless Face • Flexed Posture • Dysarthria • 30% have Cognitive impairment
Parkinson’s Disease Treatment • Lack of Dopamine (Inhibitor) • Tx: L-Dopa or Other Dopamine Enhancers • Prolonged L-Dopa Tx can result in tardive dyskinesia (increased facial and lingual movements)
Basal Ganglia Disease • Parkinson's disease: loss of dopamine in the neostriatum • Treatment: increase dopamine • Schizophrenia: Too much dopamine • Treatment: Block some (D2) dopamine receptors. • Problem: Prolonged treatment using Chlorpromazine and Haloperidol leads to Parkinson's disease-like tremors (tardive dyskinesia) Not enough DA Parkinsons ‘Normal’ Too much DA Schizophrenia