Download
1 / 1
10 likes | 159 Views
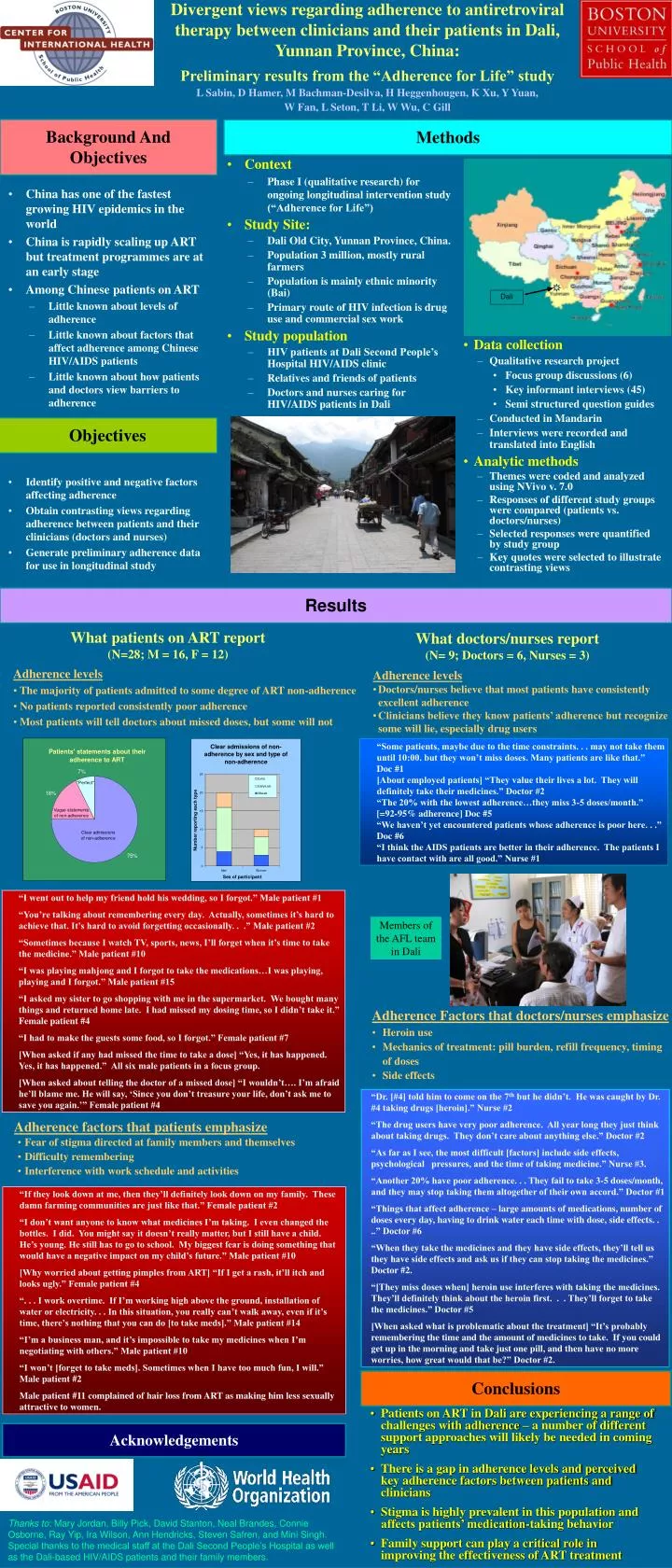
Divergent views regarding adherence to antiretroviral therapy between clinicians and their patients in Dali, Yunnan Province, China: Preliminary results from the “Adherence for Life” study L Sabin, D Hamer, M Bachman-Desilva, H Heggenhougen, K Xu, Y Yuan, W Fan, L Seton, T Li, W Wu, C Gill.

E N D
Divergent views regarding adherence to antiretroviral therapy between clinicians and their patients in Dali, Yunnan Province, China: Preliminary results from the “Adherence for Life” study L Sabin, D Hamer, M Bachman-Desilva, H Heggenhougen, K Xu, Y Yuan, W Fan, L Seton, T Li, W Wu, C Gill Background And Objectives Methods • Context • Phase I (qualitative research) for ongoing longitudinal intervention study (“Adherence for Life”) • Study Site: • Dali Old City, Yunnan Province, China. • Population 3 million, mostly rural farmers • Population is mainly ethnic minority (Bai) • Primary route of HIV infection is drug use and commercial sex work • Study population • HIV patients at Dali Second People’s Hospital HIV/AIDS clinic • Relatives and friends of patients • Doctors and nurses caring for HIV/AIDS patients in Dali • China has one of the fastest growing HIV epidemics in the world • China is rapidly scaling up ART but treatment programmes are at an early stage • Among Chinese patients on ART • Little known about levels of adherence • Little known about factors that affect adherence among Chinese HIV/AIDS patients • Little known about how patients and doctors view barriers to adherence • Data collection • Qualitative research project • Focus group discussions (6) • Key informant interviews (45) • Semi structured question guides • Conducted in Mandarin • Interviews were recorded and translated into English • Analytic methods • Themes were coded and analyzed using NVivo v. 7.0 • Responses of different study groups were compared (patients vs. doctors/nurses) • Selected responses were quantified by study group • Key quotes were selected to illustrate contrasting views Objectives • Identify positive and negative factors affecting adherence • Obtain contrasting views regarding adherence between patients and their clinicians (doctors and nurses) • Generate preliminary adherence data for use in longitudinal study Results What patients on ART report (N=28; M = 16, F = 12) What doctors/nurses report (N= 9; Doctors = 6, Nurses = 3) • Adherence levels • Doctors/nurses believe that most patients have consistently excellent adherence • Clinicians believe they know patients’ adherence but recognize some will lie, especially drug users • Adherence levels • The majority of patients admitted to some degree of ART non-adherence • No patients reported consistently poor adherence • Most patients will tell doctors about missed doses, but some will not • “Some patients, maybe due to the time constraints. . . may not take them until 10:00. but they won’t miss doses. Many patients are like that.” Doc #1 • [About employed patients] “They value their lives a lot. They will definitely take their medicines.” Doctor #2 • “The 20% with the lowest adherence…they miss 3-5 doses/month.” [=92-95% adherence] Doc #5 • “We haven’t yet encountered patients whose adherence is poor here. . .” Doc #6 • “I think the AIDS patients are better in their adherence. The patients I have contact with are all good.” Nurse #1 • “I went out to help my friend hold his wedding, so I forgot.” Male patient #1 • “You’re talking about remembering every day. Actually, sometimes it’s hard to achieve that. It’s hard to avoid forgetting occasionally. . .” Male patient #2 • “Sometimes because I watch TV, sports, news, I’ll forget when it’s time to take the medicine.” Male patient #10 • “I was playing mahjong and I forgot to take the medications…I was playing, playing and I forgot.” Male patient #15 • “I asked my sister to go shopping with me in the supermarket. We bought many things and returned home late. I had missed my dosing time, so I didn’t take it.” Female patient #4 • “I had to make the guests some food, so I forgot.” Female patient #7 • [When asked if any had missed the time to take a dose] “Yes, it has happened. Yes, it has happened.” All six male patients in a focus group. • [When asked about telling the doctor of a missed dose] “I wouldn’t…. I’m afraid he’ll blame me. He will say, ‘Since you don’t treasure your life, don’t ask me to save you again.’” Female patient #4 Members of the AFL team in Dali • Adherence Factors that doctors/nurses emphasize • Heroin use • Mechanics of treatment: pill burden, refill frequency, timing of doses • Side effects • “Dr. [#4] told him to come on the 7th but he didn’t. He was caught by Dr. #4 taking drugs [heroin].” Nurse #2 • “The drug users have very poor adherence. All year long they just think about taking drugs. They don’t care about anything else.” Doctor #2 • “As far as I see, the most difficult [factors] include side effects, psychological pressures, and the time of taking medicine.” Nurse #3. • “Another 20% have poor adherence. . . They fail to take 3-5 doses/month, and they may stop taking them altogether of their own accord.” Doctor #1 • “Things that affect adherence – large amounts of medications, number of doses every day, having to drink water each time with dose, side effects. . ..” Doctor #6 • “When they take the medicines and they have side effects, they’ll tell us they have side effects and ask us if they can stop taking the medicines.” Doctor #2. • “[They miss doses when] heroin use interferes with taking the medicines. They’ll definitely think about the heroin first. . . They’ll forget to take the medicines.” Doctor #5 • [When asked what is problematic about the treatment] “It’s probably remembering the time and the amount of medicines to take. If you could get up in the morning and take just one pill, and then have no more worries, how great would that be?” Doctor #2. • Adherence factors that patients emphasize • Fear of stigma directed at family members and themselves • Difficulty remembering • Interference with work schedule and activities • “If they look down at me, then they’ll definitely look down on my family. These damn farming communities are just like that.” Female patient #2 • “I don’t want anyone to know what medicines I’m taking. I even changed the bottles. I did. You might say it doesn’t really matter, but I still have a child. He’s young. He still has to go to school. My biggest fear is doing something that would have a negative impact on my child’s future.” Male patient #10 • [Why worried about getting pimples from ART] “If I get a rash, it’ll itch and looks ugly.” Female patient #4 • “. . . I work overtime. If I’m working high above the ground, installation of water or electricity. . . In this situation, you really can’t walk away, even if it’s time, there’s nothing that you can do [to take meds].” Male patient #14 • “I’m a business man, and it’s impossible to take my medicines when I’m negotiating with others.” Male patient #10 • “I won’t [forget to take meds]. Sometimes when I have too much fun, I will.” Male patient #2 • Male patient #11 complained of hair loss from ART as making him less sexually attractive to women. Conclusions • Patients on ART in Dali are experiencing a range of challenges with adherence – a number of different support approaches will likely be needed in coming years • There is a gap in adherence levels and perceived key adherence factors between patients and clinicians • Stigma is highly prevalent in this population and affects patients’ medication-taking behavior • Family support can play a critical role in improving the effectiveness of ART treatment Acknowledgements Thanks to: Mary Jordan, Billy Pick, David Stanton, Neal Brandes, Connie Osborne, Ray Yip, Ira Wilson, Ann Hendricks, Steven Safren, and Mini Singh. Special thanks to the medical staff at the Dali Second People’s Hospital as well as the Dali-based HIV/AIDS patients and their family members.






















