Download
1 / 58
580 likes | 759 Views
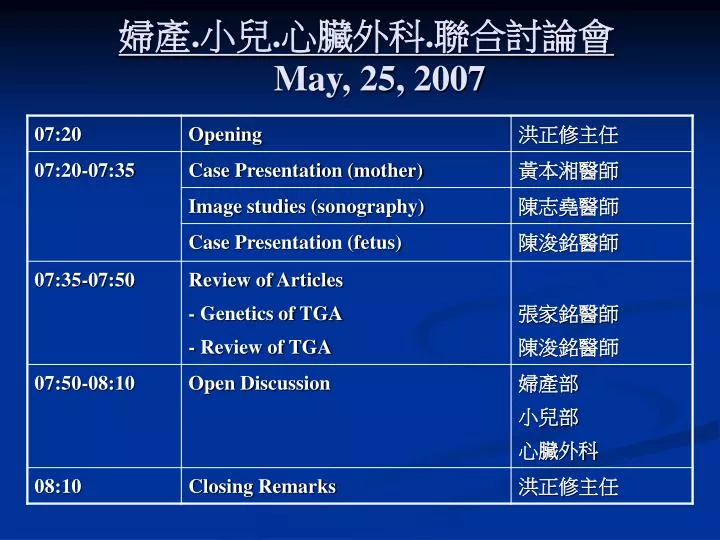
婦產 . 小兒 . 心臟外科 . 聯合討論會 May, 25, 2007. 婦產 . 小兒 . 心臟外科 . 聯合討論會. 報告:黃本湘 醫師 指導:洪正修 主任. General data. Age: 31 year-old, G2 P0 AA1 L.M.P.: 2006-06-20

E N D
婦產.小兒.心臟外科.聯合討論會 報告:黃本湘 醫師 指導:洪正修 主任
General data • Age: 31 year-old, G2 P0 AA1 • L.M.P.: 2006-06-20 • E.D.C.: 2007-03-28 • Prenatal condition: referred from LMD of preg. 24 weeks • Pre-pregnancy body weight: 54kg • Menarche: 13 years-old • Menstrual D/I: 3-4/28-30 days, dysmenorrhea (-) • Oral pills or IUD: denied • BMI: 20.1
General data General data • Marital status: married • Previous pregnancy history • No.1, 27 y/o, AA < 5 weeks Personal history • Systemic disease: denied • Surgery history: fibrocyst, right breast s/p operation in 1993 • Smoking / Alcoholism: denied • Allergy: denied
General data Family history Father is a victim of HBV carrier with liver Cirrhosis Traveling history in recent half year Italia and Singapore
Clinical course • The prenatal condition was followed up at LMD till pregnancy 24 weeks while fetal cardiac anomaly was noted. • 2006-12-07: visited CV OPD Dr. Jiang • 2006-12-11: referred to OBS OPD Chief Hong.
Clinical course • Survey for GDM: 50 gm OGT: 174 gm/dl 100 gm OGT: 75/164/140/124 gm/dl HbA1c: 4.5 • VDRL: negative • Rubella IgG: positive
Clinical course • The amniocentesis on 2006-12-11 - chromosome karyotypes:46,XY,9qh+ with normal variant • The sonography on 2006-12-15: • singleton, AGA, male, internal os: 13mm, polyhydramnios(126 x 70mm), r/o TGA and TV defect
Hospital course • The patient was ever admitted for tocolysis and antibiotics treatment due to preterm contraction and urinary tract infection (urine routine: pyuria: 2+) from 2006-12-15 to 2007-01-02. • The sonographic studying (with color doppler) on 2007-02-01, 2007-03-01, and 2007-03-08 showed AGA, with normal flow pattern, r/o TGA and TV defect. • The sonographic studying (with color doppler) on 2007-03-15 showed r/o TGA with minimal TR and pericardial effusion 1.7mm, reverse flow of DV.
Hospital course • The Cesarean section was arranged on 2007-03-21 due to the pregnancy 39 weeks fetus with transposition of great artery and pericardial effusion. • 09:21, Boy, BL: 50 cm, BW: 3108 gm, Apgar score: 6 at 1' and 9 at 5'
Hospital course Apgar score while performing baby care △- 1 minute, ○- 5 minutes
Hospital course • The boy baby was transferred to NICU for further management due to progressive cyanosis and bradycardia at DR. • The condition after the C-section was fair and the patient was discharged on 2007-03-27.
General history • 病歷號:34785xx0 • 姓名:倪xx之男 • 住院日期:20070321 • 住院號:11121xx8 • 身份性別:M • 生日:20070321
Chief complaint • D-TGV was diagnosed by fetal echocardiography when GA 24 wks
Present illness • Mother didn't have any major systemic disease before • Denied any problem during pregnancy • Regular fetal sonography revealed D-TGA when GA 24 wks
C/S was performed at 09:21 on 3/21 • Bradycardia, cyanosis after delivery • Ambu-bagging • Vital signs stable • Transfer to NICU
Brief history • Birth history • G2P1A1 • GA:39weeks • BBW:3108gm • A/P:6->9, by C/S • Family history • Grandmother: lymphoma
Physical examination • 身高:50cm(75 percentile), 體重:3.108kg(50 percentile) • Vital signs: T:35.2℃, P:140/min, R:54/min, BP:56/18mmHg • GENERAL • General appearance: moderate-developed (+) ,well-nourished (+) • HEAD • grossly normal, no trauma wound • EYES • grossly normal, no icteric sclera • EARS • Eardrum: injected(-) • NOSE • no nasal flaring • THROAT & MOUTH • injected throat(-) • NECK • supple, no lymphadenopathy, no jugular vein engorgement, no meningeal sign
SKIN • intact, pink • CHEST & LUNGS • symmetric expansion, no chest deformity, bilateral clear breathing sound • HEART • regular heart beat, no murmur • ABDOMEN • Inspection: no distention, no striaePercussion: no shifting dullness, mild tympanic soundsPalpation: no rebound pain • BACK & SPINE • no tenderness, no pits • EXTREMITIES • freely movable, no pitting edema, no clubbing finger • NEUROLOGI • sucking reflex(+), Moro reflex(+), grasp reflex(+)
Hospital course • EKG • NSR, RAD • CXR, 3/21
Echocardiography • Simple D-TGA, no VSD • No PS or AS • PDA & ASD vs PFO /c bidirectional shunt • r/o single intramural coronary artery (RCA from main LCA)
WBC : 16.3 X 1000/UL • RBC : 4.42 M/UL • HGB : 15.5 G/DL • HCT : 46.5 % • MCV : 105 FL • MCH : 35.0 PG • MCHC : 33.3 G/DL • RDW-SD : 13.8 FL • PLATELET : 282 X 1000/UL
Na 142 MMOL/L • K 4.4 MMOL/L • Bun 7 MG/DL • Cr 0.7 MG/DL • ALT 6 U/L • AST 24 U/L
Impression • Simple D-TGA • PDA & ASD vs PFO /c bidirectional shunt • r/o single intramural coronary artery • Plan • PGE1(20ug/amp) • 0.03ug/kg/min • Arrange cath
Cyanosis, mild poor activity, 1250, 3/21 • VBG: • PH: ( 7.150 ->7.169) • PO2: ( 36.0 ->29.5 ) mmHg • PCO2: ( 52.8 ->59.7 ) mmHg • HCO3: ( 18.0 ->21.2) mmol/L • BE: ( -11.1 ->-8.1) mmol/L • s/p N-P /c IMV • Sod. Bicarbonate, 3+3cc
Keep PGE1 1.5md/min(0.03ug/kg/min) • N-P with IMV->N-P->room air, 3/25 • Cath, 3/27 • Simple D-TGA • PDA & ASD • Single coronary artery, r/o intramural ca • Plan • Consult CVS for arterial switch (Jatene procedure)
Op day, 96/4/2 • Operative findings • D-TGA + intact ventricular septum • large ASD + large PDA • two coronary arteries • 1L + 2RCx combination • Operative procedure • Arterial switch operation • ASD repair
Follow up echocardiography • TGA s/p Jatene operation • Mild PS, TR • MBD on 96/4/17 due to stable condition
TRANSPOSITION OF THE GREAT ARTERIES Cytogenetic Lab. 張家銘
Frequency of cardiovascular malformations in first-degree relatives of probands with TGA Overall recurrence risk in sibs = 0.82% ( 5 in 612) • Becker et al. (1996)
levo-TGA (19) 1/50 sibs • dextro-TGA (168) 1/369 sibs and 1 father had levo-TGA • complex TGA (65) 4 /143 sibs and 2/143 parents • asplenia with TGA (19) 1/50 sibs,
mutation CFC1 gene mutation • 7-year-old girl with D-TGA and mental retardation • tandem duplication of the exon 4 splice donor site of the CFC1 gene • Goldmuntz et al. (2002)
t(12,17)(q24.1;q21), breakpoint on chromosome 12 thyroid hormone receptor–associated protein early embryonic development in various organisms THRAP2
97 D-TGA for mutations in THRAP2 • 6 intronic polymorphisms • 6 silent mutations • 4 missense mutations; disease causing, • glu251gly (608771.0001) • arg1872his (608771.0002) • asp2023gly (608771.0003) Muncke et al. (2003)
Discussion 報告者:陳浚銘 醫師 指導者:黃碧桃 醫師
Background • First described over 2 centuries ago • surgical atrial septectomy in the 1950s • balloon atrial septostomy in the 1960s • physiological repair (atrial switch operation) • anatomic repair (arterial switch operation). • survival rate > 90%
What is TGA? • Abnormal development of the fetal heart during the first 8 weeks of pregnancy • Aorta arises from the right ventricle and the pulmonary artery arises from the left ventricle
anatomic classifications of TGA • dextro-TGA [d-TGA] : • 60% of the patients, the aorta is anterior and to the right of the pulmonary artery • (arteries change) • levo-TGA [l-TGA] : • the aorta may be anterior and to the left of the pulmonary artery • (ventricles change, circulation is normal)