Download
1 / 32
320 likes | 813 Views
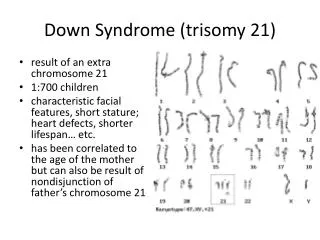
TRISOMY 21- DOWN SYNDROME. Dr. Gupta PL-II. Incidence. Approximately one in 1000 live births. Genetics. Trisomy 21 (47, +21), - 94 %, The frequency of trisomy increases with increasing maternal age.

E N D
TRISOMY 21- DOWN SYNDROME Dr. Gupta PL-II
Incidence Approximately one in 1000 live births.
Genetics • Trisomy 21 (47, +21), - 94 %, The frequency of trisomy increases with increasing maternal age. • Robertsonian translocation involving chromosome 21- Approx. 3-4 %, not related to maternal age. • Trisomy 21 mosaicism – 2 to 3 % cases
Head and neck Brachycephaly Up-slanting palpebral fissures Epicanthal folds Brushfield spots Flat nasal bridge Folded or dysplastic ears Open mouth Protruding tongue Short neck Excessive skin at the nape of neck Extremities Shortbroad hands Short fifth finger Incurved fifth finger Transverse palmer crease Space between first and second toe Hyper flexibility of joints Clinical Features
Flat facial profile Poor Moro reflex Excessive skin at the nape of neck Slanted palpebral fissures Hypotonia Hyper flexibility of joints Dysplasia of pelvis Anomalous ears Dysplasia of midphalanx of fifth finger Transverse palmer crease Neonatal features
Mental Retardation • Almost all DS babies have MR. • Mildly to moderately retarded . • Starts in the first year of life. • Average age of sitting(11 mon), and walking (26 mon) is twice the typical age. • First words at 18 months. • IQ declines through the first 10 years of age, reaching a plateau in adolescence that continues into adulthood.
Heart Disease • 50 % of Down Syndrome pts have heart disease • Atrioventricular septal defect • VSD • Secundum ASD • PDA • Tetrology of Fallot • Mitral valve prolapse • AR, MR
GI abnormalities • 5% of cases • Duodenal atresia or stenosis, sometimes assoc with annular pancreas in 2.5 % of cases • Imperforate anus • Esophageal atresia with TE fistula is less common • Hirschsprung’s disease • Strong assoc with celiac disease b/w 5 – 16 % , 5 – 16 fold increase as compared to general population
Growth • BW, length and HC are less in DS • Reduced growth rate • Prevalence of obesity is greater in DS • Weight is less than expected for length in infants with DS, and then increases disproportion ally so that they are obese by age 3-4 yrs
Eye problems Most common disorders are Refractory error – 35 to 76 percent Strabismus – 25 to 57 percent Nystagmus – 18 to 22 percent Cataract occur in 5 % of newborns. Frequency increases with age.
Hearing loss • Unilateral or bilateral • Conductive, sensorineural or mixed • Otitis media is a frequent problem
Hematologic disorders • The risk of leukemia is 1 to 1.5 percent. • 65% of newborn have polycythemia resulting in hypoglycemia. • Risk of AML and ALL is also much higher than the general population. • Transient leukemia – exclusively affects NB. - It is asymptomatic with spontaneous resolution in 2-3 months. - Vesiculopustular skin eruptions are common and resolve with disorder.
Endocrine disorder • Thyroid disease – Hypothyroidism occurs more frequently than hyperthyroidism. • Diabetes – The risk of type 1 diabetes is three times greater than that of the general population.
Reproduction • Women with DS are fertile and may become pregnant. • Nearly all males with DS are infertile. The mechanism is impairment of spermatogenesis
Atlantoaxial instability • Excessive mobility of atlas (C1) and the axis (C2), may lead to subluxation of the cervical spine. • Diagnosis made by lateral neck radiograph. • Patients are advised to avoid contact sports.
Sleep apnea • Obstructive sleep apnea is more common.
Skin disorder • Palmoplantar hyperkeratosis • Seborreic dermatitis • Fissured tongue • Cutis marmorata • Geographical tongue • Xerosis
Diagnosis • Prenatal screening • If no screening – It is recognized from the characteristic phenotypic features. • Confirmed by Karyotype.
Management 1. Growth – Measurements should be plotted on the appropriate growth chart for children with DS. • This will help in prevention of obesity and early diagnosis of celiac disease and hypothyroidism. 2. Cardiac disease – All newborns should be evaluated by cardiac ECHO for CHD in consultation with pediatric cardiologist. 3. Hearing – Screening to be done in the newborn period, every 6 months until 3 yrs of age and then annually.
Management (cont.) 4. Eye disorders - An eye exam should be performed in the newborn period or at least before 6 months of age to detect strabismus, nystagmus, and cataracts. 5. Thyroid Function – Should be done in newborn period and should be repeated at six and 12 months , and then annually. 6. Celiac Disease – Screening should begin at 2 yrs. Repeat screening if signs/Sx develop.
Management ( cont) • Hematology – CBC with differential at birth to evaluate for polycythemia as well as WBC. • Atlanto-axial instability – X ray for evidence of AAI or sub-luxation at 3 to 5 years of age. • Alzheimer’s disease – Adult with a Down Syndrome has earlier onset of symptoms. When diagnosis is considered, thyroid disease and possible depression should be excluded.
Mortality Median age of death has increased from 25 yrs in 1983 to 49 yrs in 1997, an average of 1.7 yrs increase per year. Most likely cause of death is CHD, Dementia, Hypothyroidism and Leukemia. Improved survival is because of increased placements of infants in homes and changes in treatment for common causes of death. Survival is better for males and blacks.
Counseling • May begin when a prenatal diagnosis is made. • Discuss the wide range of variability in manifestation and prognosis. • Medical and educational treatments and interventions should be discussed. • Initial referrals for early intervention, informative publications, parent groups, and advocacy groups.