Download
1 / 28
280 likes | 450 Views
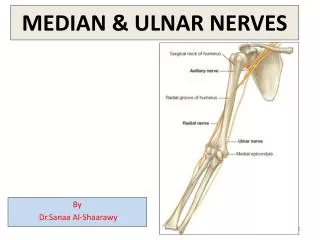
Ulnar Collateral Ligament Rehabilitation. By: Michael Cox. Bony Anatomy . Humerous : Medial epicondyle- trochlea which serves as the axis of rotation for ulna on the humeorus Lateral epicondyle- capitellum which serves as the axis of rotation for the radius

E N D
Ulnar Collateral Ligament Rehabilitation By: Michael Cox
Bony Anatomy • Humerous: Medial epicondyle- trochlea which serves as the axis of rotation for ulna on the humeorus Lateral epicondyle- capitellum which serves as the axis of rotation for the radius Radial fossa- accepts radial head during flx Coranoid fossa- accepts coranoid process during flx Olecronon fossa- accepts olecronon during ext • Ulna: Olecronon process Coranoid process • Radius: Radial head Radial tuberosity
Bony Anatomy • Humeroulnar joint Hinge joint Strong and stable Allows for flexion and extension • Humeroradial joint Modified ball and socket joint • Proximal radioulnar joint Allows for pronation and supination
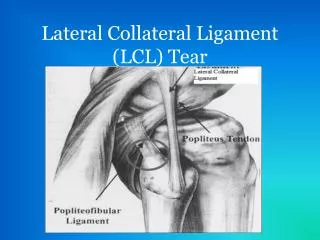
Ligamentous support • Ulnar Collateral Ligament: • Resists valgus loads • 3 bundles • Anterior- taut throughout full ROM, primary restraint against valgus stress • Transverse- provides little medial support • Posterior- taut in flexion beyond 60 degrees • Lateral Collateral Ligament: • Resists varus forces • Composed of radial collateral ligament, • lateral ulnar collateral ligament, • annular and accessory ligament • Annular Ligament: Encases radial head Doesn’t let ulna and radius move into flexion and extension independently
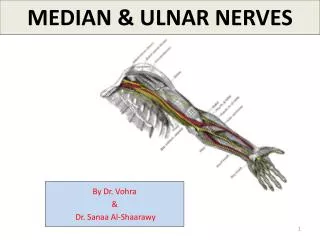
Musculature • Flexors: • Biceps brachii, brachioradialis, brachialis • Extensors: • Triceps brachii, anconeus • Forearm Pronators: • Pronator teres, pronator quadratus • Forearm Supinators: • Supinator, assisted by biceps and brachioradialis
Mechanism of Injury • Most ulnar collateral ligament injuries occur in overhead throwing athletes • This due to the extreme valgus stress placed on the elbow throughout the throwing motion • Acutely the UCL can also be injured with a lateral blow to the elbow
Clinical Evaluation • The patient will complain of pain on the medial aspect of the elbow that increases with motion • Tingling or numbness may be present due to the tensile force placed on the ulnar nerve • Point tender from the along the medial epicondyle • Some swelling may be noticeable • Positive valgus stress test
Acute treatment • Refer patient for a MRI • Restrict any throwing movements • Can sling if more comfortable • Modalities can be used to help reduce pain and inflammation such as ice and electrical stimulation for gate theory pain control
Surgical Patients • If surgery Is needed- “Tommy John”- usually uses palmaris longus tendon as a graft to replace UCL • Immobilization wit the arm at 90 degrees of flexion for 10-14 days • At this time wrist and finger ROM exercises can be started • Gripping exercises with puddy • Shoulder ROM
Beginning Rehabilitation Weeks 0-3 Goals: • Decrease pain and inflammation • Improve ROM • Retard atrophy
Early Rehab- Passive ROM • Passive extension with dumbbell hanging off table (towel under joint) 2 lbs.for 5-7 minutes (long duration, low intensity stretch) • Pulley flexion and extension 3 sets- 10 repetitions • Clinician passive ROM
Early Rehab- Active ROM Wand exercises: 3 sets- 10 repetitions flexion extension pronation supination Wrist ROM Active ROM flexion, extension, pronation, supination
Early Rehab- Decreasing Pain • Joint Mobilizations- grade I and II oscillations- posterior glide • Ice • Electrical Stim - gate theory
Early Rehab- Strengthening • Isometrics • flexion, extension, pronation, supination • 3 sets of 10 repetitions holding contractions for about 5-10 seconds • Refrain from internal and external rotation due to the valgus stress it places on the UCL
Intermediate Rehabilitation Weeks 4-8 Goals: • Improving strength and endurance • Reestablishing neuromuscular control • Maintain full ROM • Criteria: Near total ROM with minimal pain
Intermediate Rehabilitation Isotonic exercises Flexion extension pronation supination 3 sets- 10 repetitions Starting at 2lb dumbbell and progressing as strength increases Wrist isotonic exercises Rhythmic Stabilization clinician assisted swiss ball 4 sets- 20s
Intermediate Rehabilitation Diagonal PNF patterns Body Blade straight arm and at 90
Moderate Rehabilitation Weeks 9-13 Goals: • Advanced strengthening phase • Increase total arm strength, power, endurance, and neuromuscular control • Prepare patient for functional return to play activities Criteria: • Full non painful ROM • Strength close to 70% of uninvolved limb
Moderate Rehabilitation • Eccentric training • Theraband- biceps and triceps
Moderate Rehabilitation • Throwers 10- total arm strength • Dumbbell abduction • Prone dumbbell abduction • Prone extension • Internal rotation • External rotation • Theraband shoulder flexion and extension • Progressive pushups • Medicine ball punches- serratus anterior • Diagonal D2 PNF • Wrist flexion, extension, pronation, supination
Moderate Rehabilitation • Plyometrics • Med ball throws one hand • Soccer throw • Chest pass • Side to side Plyometric press up
Moderate Rehabilitation • Progressive medicine ball plyometrics • Increased soccer throws • 8-10 reps • Side hits • 2 sets- 30 seconds • External rotation throws • 3 sets- 10 reps
Final Rehabilitation Weeks 14-26 Goal: • Progressive functional drills • Continue to increase strength, endurance, power • Return to play Criteria: • Full ROM with no pain • Full strength
Final Rehabilitation • Throwing program • Increase in distance and amount of throws • Enough rest time in-between session: 2-3 days Batting practice • Tees • Soft toss • Slow pitching • Against a pitcher
Return To Play • Full ROM • Full strength • No direct pain with throwing or hitting • Normal cardiovascular endurance • Physiologically ready
Article • Emphasizes maintaining full elbow extension early • Important to strengthen elbow and wrist flexors, and pronators- importance in follow through phase • Rotator cuff strength • Progressive and essential rehabilitation program
Summary • Elbow joint has strong bony support as well as ligamentous and capsular support • Mechanism of injury is usually repetitive valgus stress • Progressive rehab with certain criteria that must be met before moving on • Avoid internal and external rotation early in rehab due to valgus stress it places on elbow • Maintain cardiovascular endurance and core strength throughout rehab • Flexibility • Continue strengthening once back to full participation to decrease risk of re-injury
Questions ??????????