Download

1 / 39
400 likes | 696 Views
Tendon Injuries: New Treatments For an Old Problem. Ken Mautner , MD Emory Sports Medicine February 12, 2009. Tendon Injury – Terms. Tendinitis Implying inflammatory pathology Tendinosis Implying degenerative pathology w/o inflammatory component Tendinopathy

E N D
Tendon Injuries: New Treatments For an Old Problem Ken Mautner, MD Emory Sports Medicine February 12, 2009
Tendon Injury – Terms • Tendinitis • Implying inflammatory pathology • Tendinosis • Implying degenerative pathology w/o inflammatory component • Tendinopathy • No implication for pathology
Tendon Structure Tropocollagen Triple Helix Structure
The Tendinopathy Cycle http://www.clinicalsportsmedicine.com/articles/common_tendinopathies.htm
Tendinosis Microscopic Collagen degeneration Fibrosis Neovascularization LACK of inflammation Normal Tendinosis J.D. Rees et al, Rheumatology May 2006
LACK OF EVIDENCE FOR TRADITIONAL TREATMENTS What is ideal way to treat tendinopathy? • Traditional Treatments • Rest • Immobilization • NSAIDS • Physical Therapy/ biomechanics • Possible CSI • RTP when pain free/ functional • But is tissue healed? • If symptoms persist • Surgery
TIMING OF INTERVENTION AND TYPE OF INTERVENTION NEEDS MORE EVIDENCE What is ideal way to treat tendinopathy? • Evolving algorithm • Pathology specific conservative treatments • NSAIDS only if inflammatory • Immobilization only if necessary • Eccentrics exercises for tendinosis • Regenerative intervention • Percutaneous needle tenotomy • PRP • PRP with adipose tissue • BMAC • Cultured stem cells
Evolution of Regenerative Injections for treating chronic tendinopathy Proliferative therapy (prolotherapy) was first described in the 1930’s and represents first form of regenerative medicine Theory is that irritant solutions (most often dextrose) along with needling of soft tissues stimulates an inflammatory reaction which initiates a healing cascade for injured soft tissues. This technique has been employed for chronic enthesopathies and ligamentous injuries/laxity.
PercutaneousTenotomy (PNT) • Release of tissue by repetitive needling of a tendon insertion will induce inflammation, a release of growth factors which leads to fibroblast proliferation and ultimately healing
Evolution of platelets for healing soft tissue injuries First use of PRP in US was in 1987 following open heart surgery Periodontal and wound healing were early successful clinical applications of PRP Benchwork research has clearly demonstrated proliferation of GF’s with supraphysiologic amount of platelets Prior to human use, considerable use and success in Equine (horse) racing with tendon regeneration using PRP
The “perfect storm” for clinical application of platelets in MSK injuries • Rapid growth of ultrasound use in MSK medicine • Ease of obtaining and using Platelets without the need for OR/ ASC • Unsuccessful traditional treatmentments of tendonopathy/chronic soft tissue injuries • Motivated patient population (athletes) that will do anything to get back sooner/ stronger • Early pilot studies/ case series showing remarkable success of procedure and the ability to “fix” an injury without surgery • What’s the downside?
Why do we need to concentrate platelets? Studies have shown accelerated would healing requires at least 4x-5x platelet concentration An exponential increase in cell proliferation occurs as platelet concentration increases from 2.5x to 5x-10x baseline levels Much lower volume needed to get high levels of platelets to area
PRP for chronic lateral epicondylosis • Allan Mishra et al, AJSM, 2006 • 140 pts evaluated for lateral epicondylosis • 20 had refractory pain an avg. of 15 months later • 15 in treatment group, 5 in bupivicaine control group • Intervention • Injection w/ autologous PRP once into common extensor tendon followed by gradual increase in rehab program through 4 weeks after which full activity allowed • Outcome • A 46%, 60% and 81% improvement in VAS pain scores at 1, 2 and 6 months respectively in tx group • 3/5 in bupivicaine group withdrew/ sought other tx • At final F/U (12-38 months) 93% pain free (<10/100 VAS) • No complications, no one got worse
PRP vs Steroid Injection for Lateral Epicondylitis • Peerbooms et al, AJSM, February 2010 • Double blind RCT with 1 year follow up of 100 pts • No Ultrasound guidance was used • Success defined as >25% reduction in VAS or DASH score • RESULTS • At 1 yr, 49% of CSI group and 73% in PRP group were successful (p<.001)
Short axis view PRP lateral epicondylosis- Case #1 Long axis view
Elbow case #1– 2.5 months later BEFORE AFTER
Elbow case #1– 2.5 months later BEFORE AFTER
AFTER (3 months) Elbow PRP Case #2 BEFORE
PRP for Achilles Tendinosis • de Vos et al, JAMA, January 13, 2010 • First double blind, placebo controlled, RCT on PRP • 54 randomized patients age 18 to 70 with chronic (at least 2 mo) achilles tendon pain 2 to 7 cm above calcaneus • Either 6cc PRP or Saline was injected with US guidance into achilles tendon • Rehab for both groups involved rest and then after 2 weeks, started on 12 week daily (180 repetitions) eccentric exercise program • No sports for at least 4 weeks and then only if pain <=3/10 • f/u qestionnaire at weeks 6,12,24
PRP for Achilles Tendinosis • de Vos et al, JAMA, January 13, 2010 • RESULTS • After 24 weeks, no statistical difference between the 2 groups • Both groups improved > 20 pts on VISA-A scores (0-100) • No adverse events in either group (ruptures/ infections) • CONCLUSIONS • Both groups improved • Needle? Saline? Placebo? Eccentric Exercises? • Only 1 treatment done • Small Sample Size • Eccentric exercises may have worsened outcomes • Certainly this confounded the results
PRP for Achilles Tendinosis • Gaweda K et all . Treatment of Achilles Tendinopathy with Platelet-Rich Plasma, International J. of Sports Medicine, 2010 • 14 patients (15 tendons), prospective study • Avg. 6 months symptoms (range 3-10 months) • 3 cc PRP injected under US guidance • Rehab –PWB x 3 days, PROM x 2 wks, then active ROM, stretching from 2-6 wks, then >6wks, full load active exercises • Results • Tendon thickness decreased in 13/15 tendons by 6 months • Intrasubstance tears reduced from 11/15 to 1/15 at 6 mo.
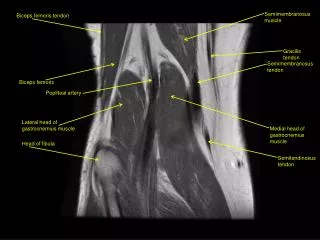
Achilles Tendon Pain Longitudinal achilles Short axis achilles
Achilles PRP Injection8 months later BEFORE AFTER
Achilles PRP Injection8 months later BEFORE AFTER
Preliminary Results of PRP Surveyfor chronic tendinopathyDATA COLLECTION STILL ONGOING • Multi-center study • 146 patients sent questionnaire (as of oct. 1) • 94 responded (64%) • 71/ 94 (76%) were isolated treatments for tendinopathy • 22/67 (33%) tendons received a 2nd PRP injection (all within 4 months of the first injection) • All retrospective data analyzed with following questions: • VAS score –pre and post • Overall improvement • Not at all, slightly, moderately, mostly, completely • Overall satisfaction
Distribution of tendons (responders only) 19 -- Common extensor tendon at lateral epicondyle 15 -- Patella Tendon 10 – Rotator cuff 6 – Gluteus medius/ minimus 6 – Achilles tendons 4 – Common flexor tendon at medial epicondyle 3 -- Hamstring
Pain Score pre and post PRPtendons only 7.4 2.4 ➤ 68% Reduction in VAS
Overall Improvement 79% reported moderate to complete improvement – 50%- 100% relief of symptoms 59 % reported mostly to complete improvement -- 75-100% relief of symptoms
Overall Improvement Percentage 95% moderate to complete improvement 60% moderate to complete improvement 90% moderate to complete improvement
Overall satisfaction with PRP procedure DATA COLLECTION STILL ONGOING
Conclusion • Tendon injuries have had poor clinical success with traditional treatments • Some will improve on there own, but will the tendon regain its normal architecture/ strength? • Biological agents such as PRP may offer a way to cure chronic tendon pain • Techniques will be refined over next several years
Thank You Ken.mautner@emory.org
Rehabilitation after PRP • Days 0- 3 • Ice allowed for first 24 hrs only as needed (20 min at a time) • Protected weight bearing for lower extremity procedures (walking boot) • Rest from all use of affected extremity beyond necessary daily activities • Take tylenol or hydrocodone as needed (avoid anti-inflammatory (NSAID’S) medications, e.g. ibuprofen, aspirin) • Days 4-14 • Wean out of boot/ splint • Light biking or pool work allowed (stay below pain) • Take Tylenol as needed (avoid NSAID’S) • Weeks 2-4 • Continue bike/pool work • Resume formal physical therapy/ rehabilitation to include: • Light stretching • Soft tissue work (including CFM, ASTYM, Graston, ART) • Heating/ ultrasound modalities • Core work/ strengthen adjacent body parts • Shoulder and scapulo-thoracic work for elbow procedures • Hip/ core work for knee and foot/ankle procedure • May walk lightly for exercise on treadmill/ flat ground if no increase in pain
Rehabilitation after PRP • Weeks 4-8 • Advance formal physical therapy/ rehabilitation: • Eccentric exercises – start with light weight • Re- Introduce strengthening exercise • Lower extremity closed kinetic chain exercises allowed with light weights/body weight • Continue light aerobic/ weight bearing exercise (if little to no pain present) • Start slow and do no more than every other day initially with small increases each time if no increase symptoms. • Months 2-6 • Advance formal physical therapy/ rehabilitation: • Increase strengthening activities (esp. eccentrics) • introduce dynamic stabilization and integrated musculoskeletal activities • Increase aerobic activities slowly • May start to resume sport specific activities ONLY IF PAIN IS MINIMAL with these activities • Start out with no more than every other day and increase amount of activity slowly each time if activity does not cause pain and no increase pain after activity is done • Progress sporting activities as tolerated to full return to play!! • If additional procedures are done, the rehabilitation starts over with the additional procedure