Download
1 / 47
490 likes | 590 Views
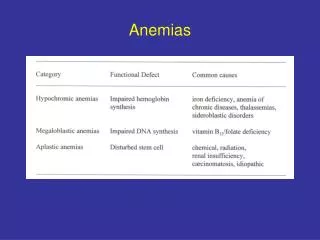
MACROCYTIC ANEMIAS. Anemias where the RBC are larger than normal. Macrocytic anemias are classified as megaloblastic & non-megaloblastic. Megaloblastic anemia. the most common cause of macrocytic anemia

E N D
MACROCYTIC ANEMIAS Anemias where the RBC are larger than normal
Macrocytic anemias are classified as megaloblastic & non-megaloblastic
Megaloblastic anemia • the most common cause of macrocytic anemia • is due to a deficiency of either vitamin B12,folic acid (or both). • Pernicious anemia is caused by a lack of intrinsic factor
Megaloblastic anemia • associated with defective DNA synthesis • and therefore, abnormal RBC maturation in the marrow (a nuclear maturation defect).
Megaloblastic anemia Primary defect in DNA replication is due to depletion of thymidine triphosphate which leads to retarded mitosis, therefore retarded nuclear maturation. Cytoplasmic maturation proceeds ahead of nuclear maturation Nuclear/cytoplasmic asynchrony
Megaloblastic anemia the granulocytic & megakaryocytic maturation are also affected, this leads to pancytopenia
Vitamin B12 • Intrinsic factor (IF) – produced in the stomach • Vitamin B12 & IF complex binds to mucosal cells in the ileum & enters. • B12 is released from the mucosal cell, • it binds to transport proteins (transcobalamin) in the blood • B12 is transported to the bone marrow for use or to the liver for storage.
VITAMIN B12 ABSORPTION Mucosal cell
Requirement • Humans need 3-5 ug/day of vit B12 • Since only 70% of dietary B12 is absorbed, the diet needs to contain 5-7 ug/day. • Decreased vitamin B12 therefore results in no conversion of N5-methyl THF to THF. Thus, the net result is that dTMP for DNA synthesis is not made.
Requirement Vitamin B12 (cyanocobalamin) is found in meats, eggs, dairy products, liver. • Humans need 3-5 ug/day of vit B12 • Since only 70% of dietary B12 is absorbed, the diet needs to contain 5-7 ug/day.
MEGALOBLASTIC ANEMIAS • Therefore, with decreased folic acid, the net result is the same as that for decreased vitamin B12 – there is decreased conversion of dUMP to dTMP, and thus, dTTP which is required for DNA synthesis. • Defective DNA synthesis may occur when dUTP gets used in place of dTTP because there is a great increase in erroneous DNA copying where dUTP is put in place of dTTP. • Humans need to get about 50 ug/day of folic acid from the diet
Causes of Vit.B12 deficiency 1. Malabsorption 2. Inadequate intake 3. Inadequate utilisation
Causes of Vit.B12 deficiency 1. Malabsorption a) Inadequate production of intrinsic factor pernicious anemia - gastrectomy - atrophy of gastric mucosa b) Inadequate release of vit. B12 from food c) Terminal ileum disease d) Competition for intestinal B12 : - bacterial overgrowth e)Defective or absent transport protein (transcobalamin)
Causes of Vit.B12 deficiency 2. Inadequate intake - vegans 3. Inadequate utilisation Drugs
PERNICIOUS ANEMIA • vitamin B12, due to a def of IF • 60-70 years, rare before 40 years • Auto-immune pathology, parietal cells & IF antibodies
Three types of autoantibodies • Type I (75%)- that blocks the binding of vitamin B12 to intrinsic factor. • Type II - prevent binding of the intrinsic factor–vitamin B12 complex to its ileal receptor. • Type III (85-90%) recognize the α & β subunits of the gastric proton pump not specific
CLINICAL Anemia with variable severity Mild jaundice Neurological Myelitis => paraplegia. Pyramidal & posterior column lesions. Digestive Glossitis Dyspepsia Diarrhea
Folic acid (pteroyl glutamic acid) • found in most foods, • abundant in green leafy vegetables • eggs, milk, yeast, liver. • destroyed by heat • Absorption occurs in duodenum & jejunum • need about 50 ug/day of folic acid
Causes of Folic acid deficiency 1. Inadequate intake 2. Malabsorption 3. Increased requirement 4. Defective utilisation
Folic acid deficiency 1. Inadequate intake - diet lacking fresh food; chronicalcoholism, total parenteral nutrition, 2. Malabsorption - small bowel disease - alcoholism
Folic acid deficiency 3. Increased requirement - pregnancy, lactation - infancy - chronic hemolysis - hemodialysis 4. Defective utilisation drugs D. Excess urinary folate loss
MEGALOBLASTIC ANEMIAS • In both types of deficiency the symptoms include pallor, weakness, lightheadedness, a smooth, sore tongue, and diarrhea alternating with constipation • In vitamin B12 deficiency, there are neurological disturbances including numbness and tingling of extremities, gait abnormalities, and mental disturbances. • Older theories suggest that the B12 deficiency leads to a defect in the degradation of propionyl CoA to succinyl CoA leading to an accumulation of propionyl CoA:
MEGALOBLASTIC ANEMIADiagnosis 1. Diagnosis of megaloblastic anemia 2. Establishing the type of deficiency (vit. B12 and/or folic acid) 3. Establishing the cause of deficiency
MEGALOBLASTIC ANEMIAS • Lab findings • Macrocytic, normochromic anemia (MCV=100-140, MCHC is normal)) • MCH is increased (due to increased cell size) • Hemoglobin & RBC counts are decreased • WBC & platelet counts are decreased
MEGALOBLASTIC ANEMIAS peripheral smear, a triad of findings is commonly seen: oval macrocytes, Howell Jolly bodies (nuclear DNA fragments), hypersegmented neutrophils (5 or more lobes).
Peripheral Smear - Megaloblastic Anemia Hypersegmented neutrophil
MEGALOBLASTIC ANEMIAS peripheral smear, nucleated RBCs, polychromatophilia, The absolute reticulocyte count is decreased because of ineffective erythropoiesis.
BONE MARROW PICTURE Hypercellular Megaloblasts Giant band forms Giant metamyelocytes Abnormal megakaryocytes with multilobated nuclei
Megaloblast(vs Normoblast) abnormal, large, nucleated erythroid precursors, having nuclear-cytoplasmic asynchrony i.e. nuclear maturation lags behind that of cytoplasm The nuclei are large, having fine, reticular and open chromatin that stains lightly
MEGALOBLASTIC ANEMIAS The bone marrow will show hypercellularity, yet there are decreased numbers of all cell types in the peripheral blood (pancytopenia) because of ineffective hematopoiesis & many cells are dying prematurely in the bone marrow.
Biochemical changes – rise in serun unconjugated bilirubin & LDH
Special tests • Serum vitamin B12 assay • Schilling test • Urinary excretion of FIGLU • Serum folate essay • Red cell folate essay
MEGALOBLASTIC ANEMIAS In B12 deficiency –decreased serum vitamin B12 In folic acid deficiency –decreased serum & RBC folate
MEGALOBLASTIC ANEMIAS Specific tests for PA • Gastric analysis – if there is no free HCl after histamine stimulation, this may indicate PA since the same cells that secrete HCl, also secrete intrinsic factor (IF) • Test for antibodies to IF
Megaloblastic Anemia Other Labs • Homocysteine – Folate def. • Methylmalonic acid – B12 def. • Schilling test
SCHILLING TEST low
MEGALOBLASTIC ANEMIA Endoscopy : • Atrophic gastritis • Intestinal metaplasia
Macrocytic anaemia -Non-megaloblastic • Haemolysis • Liver disease • Alcoholism • Hypothyroidism • Aplastic anaemia • Myeloproliferative disorders • Reticulocytosis