Download
1 / 21
210 likes | 254 Views
Investigating the alterations in plaque morphology by intensive statin treatment and its relation to lipid changes, macrophage functionality, and transcriptomes. The research aims to examine lipid content changes in obstructive lesions and correlate with morphological alterations. It involves high-dose statin therapy and analyses using NIRS, OCT, and PBMC transcriptomes. The study population consists of patients with two/three vessel CAD undergoing imaging before and after statin therapy. Results show improved plaque stability, macrophage functionality, and reduced inflammation after treatment. Genes related to cholesterol synthesis, fatty acid regulation, and cholesterol metabolism were found to play key roles. The study highlights the benefits of intensive statin treatment on plaque stabilization and vascular health.

E N D
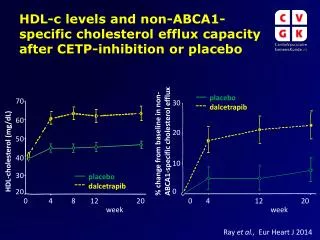
Intracoronary imaging, cholesterol efflux and transcriptomes after intensive statin treatment YELLOW II(Reduction in Coronary Yellow Plaque, Lipids and Vascular Inflammation byAggressive Lipid Lowering) Annapoorna Kini, MD, MRCP, FACC Director, Cardiac Catheterization Lab Director, Structural Heart Disease Program Director, Interventional Cardiology Fellowship Program Zena and Michael A. Wiener Professor of Medicine Cardiovascular Institute Mount Sinai Hospital, New York, NY
Disclosure Statement of Financial Interest This research was conducted with support from the Investigator-Sponsored Study Program of AstraZeneca, partial support from Infraredx and Mount Sinai catheterization laboratory endowment funds
Hypothesis Plaque morphologycan be altered by high-dose statin therapy and the changes will be related to alterations in LDL-C, HDL-C, Apo-AI, and macrophagefunctionality resulting from these lipid changes Primary End-points: To examine changes in lipid content of the obstructive non culprit lesion (NCL)measured by NIRS and plaque morphology assessed by OCT and To compare the changes in lipid content and plaque morphology to the changes in LDL-C, HDL-C, Apo-AI and macrophage functionality Secondary End-point: Correlations between the changes in plaque morphology, CEC and perturbations in PBMC transcriptome.
Methods Total number of patients screened: N = 962 Generally/clinically excluded:N = 31 Renal insufficiency, participating in another study Angiographically excluded:N = 834 Normal coronaries, non-obstructive or 1 vessel CAD, ISR, CTO, vein graft Patients excluded based on NIRS: N = 6 Study lesion maxLCBI4mm <150 Lost to follow-up: N = 6 Final study population: N = 85
Two/Three Vessel CAD After culprit vessel PCI, NCL underwent NIRS/IVUS maxLCBI4mm < 150 -> EXCLUDE maxLCBI4mm ≥ 150 -> OCT Rosuvastatin 40 mg daily (8-12 weeks) Imaging data analysis, CEC assessment and PBMC microarray by independent core labs Follow-up Cath and PCI of NCL (angiogram, OCT and NIRS/IVUS) Clinical follow-up at 1, 6, 12 month
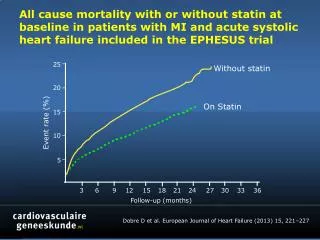
Correlates of change in FCT stratified by use of statin at baseline
Intravascular imaging Baseline: Follow-up:
Gene expression profiling • A total of 29,377 probes mapping to 20,819 genes were assayed using Microarray technology (Illumina Human HT-12 v4 bead chip array) • After data normalization, quality control and removing non-expressed genes 9,981 probes mapping to a total of 9,978 genes were retained to identify the differential expression profile • The differential expression profile identified 117 genes with 78 upregulated and 39 downregulated genes
Genesassociated with favorable outcomes SQLE- catalyzes the first oxygenation step in sterol biosynthesis, one of the crucial rate-limiting enzymes in this pathway (Howe et al. J Biol Chem2015;290:27533-44) DHCR24 - terminal enzyme in the cholesterol synthesis and a mediator ofvascular inflammation inhibition by lipid-free ApoAI(Luu et al. J Lipid Res 2014;55:410-20; Wu et al. Circ Res2013;112:278-88) FADS1 - regulation of fatty acids unsaturation LDLR- cellular cholesterol uptake ABCA1, ABCG1 - cholesterol efflux
Integrated molecular network of modules and biochemical functions mediating CEC and FCT N=37
Projection of WGCNA module genes associated with CEC to human pathways
Projection of WGCNA module genes associated with FCT to human pathways
CONCLUSIONS • We detected a significant increase in FCTof obstructive coronary lesions by OCT, enhancement of CEC, reduction in CRP level and significant perturbations in PBMC transcriptome after 8-12 weeks of rosuvastatin 40 mg daily. • Improved macrophage CEC and reduced CRP contributed to plaque stabilization independently of changes in serum cholesterol. • The significant transcriptomic perturbations related to cholesterol synthesis (SQLE), regulation of fatty acid unsaturation (FADS1), cellular cholesterol uptake (LDLR), efflux (ABCA1, ABCG1)and inflammation (DHCR24)may co-operate in determining the beneficial effects of statin on plaque stabilization.
Maximized Statin Treatment PBMC transcriptomic perturbations (SQLE, FADS1, LDLR, ABCA1, ABCG1, DHCR24) Improved CEC Reduced hs-CRP Stabilized plaque Vulnerable plaque
Thank you!!! Mount Sinai Hospital and Icahn School of Medicine at Mount Sinai, New York, NY: Vengrenyuk Y, Purushothaman M, Yoshimura T, Aquino M, Haider N, Feig J, Krishnan P, Sweeny J, Mahajan M, Moreno M, Mehran R, Kovacic J, Baber U, Narula J, Sharma S Shameer K, Johnson K, Readhead B, Kidd B, Dudley J Maehara A, Matsumura M Icahn Institute for Genomics and Multiscale Biology, Icahn School of Medicine at Mount Sinai, New York, NY: Columbia University Medical Center and CRF, New York, NY: