Download
1 / 23
230 likes | 366 Views
Policy Midterm Assignment. Winter 2011 Advanced Policy SW 8770 Maricar Tan.

E N D
Policy Midterm Assignment Winter 2011 Advanced Policy SW 8770 Maricar Tan
The Southeastern Michigan region, which includes the City of Detroit and Wayne, Oakland, Macomb, Monroe, Lapeer and St. Clair Counties, is home to 44% of the State's population but accounts for 67% (12,370) of Michigan's estimated cases of HIV. The City of Detroit makes up 9% of Michigan's population, but 39% (5,401) of the State's reported cases of HIV/AIDS (CHAG Detroit 2010). HIV/AIDS in the Metro Detroit Area
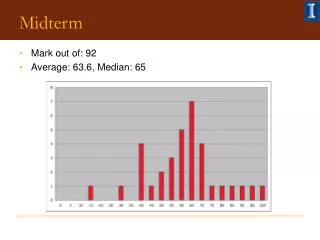
The Michigan Department of Community Health reports that each year, there are more new diagnoses of HIV infection than deaths. People that are living with HIV in Michigan is increasing. Social Problem:How can we reduce the number of people being infected by HIV in the Metro Detroit area?
Social Problem • What can we do to reduce the number of people being infected by HIV in the Metro Detroit area? • Possible Solution • Target high risk population by education and outreach and access to adequate and medical care with interventions that are culturally sensitive and appropriate to the community A Possible Solution
Strategies and interventions How to recruit and retain HIV positive people into care
This article discusses the success of using indigenous outreach workers of varying ethnicities whom many had experience with drug use and some had lived in the community being served. They would bring HIV interventions out to the target populations. One of the problems with project recruitment is that subjects are often reluctant to participate and had little motivation to do so. The outreach workers had to overcome the idea that the outreach was a finite contract for study purposes. Although food and cash were used as incentives for this which may not be realistic in continuing, the article makes a point to say that they rates for follow up were incredible for IV and crack users. Additionally, the ability of the outreach workers, former drug users themselves, to reach and recruit participants was critical to the study’s success. Their experiences made it easier to reach this population. The use of HIV positive peers as a part of outreach could help others with HIV and show them that HIV can be successfully managed. Andersen, M., Booth, R., Smereck, G., Tinsley, J., Ross, D., Haith, D., ... Matzger, H. (1998). Community outreach with active drug users: The Detroit experience. AIDS and Behavior, 2(1).
This article discusses an innovative intervention and service delivery model used by a clinic in Detroit that specifically targets in assisting underserved women with HIV who also have a history of substance abuse and mental illness. Providers “hyperlink” or get direct access for women into care through personal contacts instead of the consumers getting lost in searching for a provider and slow procedures in getting appointments. The article also discusses overcoming other barriers to care like transportation and child care. What is particularly useful is the LIGHT model of care that is used in approaching clients. This is critical to success of follow up to care with the patients. They often have low self esteem and do not feel they are entitled to care. By improving their sense of well being, they are more likely to have both interest and energy in taking care of their health. This article is a good example of how integrated care shows promise and success for those who have multiple diagnosis, something likely for citizens of Detroit. The resources that the clinic provided for the clients were rather extensive especially in terms of providing transportation, one of the highest barriers in getting care. It maybe unrealistic that this service could be provided and staffed sufficiently. This article does promote a different practice perspective that could be effective in helping prevent infection of HIV and retain patients into care. This article is also reliable in its source as a peer reviewed journal. Andersen, M. D., Smereck, G., Hockman, E. M., Ross, D. J., & Ground, K. J. (1999, March/April). Nurses decrease barriers to health care by “hyperlinking multiple-diagnosed women living with HIV/AIDS into care. Journal of the Association of Nurses in AIDS Care, 10(2), 55-65.
This article examines a policy for recalcitrant behavior among people who are living with HIV/AIDS. Local health departments are to investigate allegations that people who have HIV are engaged in behavior that would spread HIV. There is a series of steps that take place if a person is suspected to be recalcitrant. The person is issued a warning letter mandating that high risk behavior cease and maybe required to go to the local health authority for counseling and additional testing. If a person fails to respond to the warning notice, that person maybe brought into court and with only a preponderance of evidence, a judge can deem a person a Health Threat to Others (HTTO) and order up to a six month detention. The argument that this article is proposing is that once a warning notice has been issued, the person in question will have their name placed on a list and other additional information in a case that helps local public health identify those deemed to be a possible HTTO. Under policy guidelines, the warning notice cannot be contested before it is sent out. This is not unlike another article mentioned here about how partner notification can be detrimental to helping stop HIV’s spread. This list could be viewed as a breach of civil liberties. This article presents AIDS activists’ concerns with this policy. This source was helpful because it does again address concerns that people with HIV will be further discriminated against. This policy attempts to contain the HIV threat while also punish the HIV carrier. Heywood, T. A. (2010). State health policy raises red flags for HIV activists. Retrieved from http://michiganmessenger.com/44590/state-health-policy-raises-red-flags-for-hiv-activists
This article examines the barriers that would stop a person who is HIV positive into getting into case management, specifically those who are without primary care in an urban area. These barriers are important to identify so that any future programs to help reduce HIV infection may take them into consideration. Often people who are seeking medical assistance need assistance in other areas as well, such as basic needs like food and transportation. Getting them linked to case management would beneficial for them because it would can address both medical and social needs. There is an inverse relationship to lack of medical care and case management. The lack of medical care could be an a barrier to case management. The most significant factor appeared to be substance abuse. Clients that requested substance abuse treatment needed also basic needs assistance. People who abuse substance often have different motivations and it can interfere with case management. One of the reasons why this article was important to advocacy is because it looks at reasons why people may not receive the services that they may need. It does not change my view on prevention of HIV. This article does note its limitations as only association and not causality are determined. The majority of the study did rely on self report which can be biased. Substance use can be underreported in these circumstances due to stigma and legality concerns. Johnson, D., Polansky, M., Matosky, M., & Teti, M. (2010). Psychosocial factors associated with successful transition into HIV case management for those without primary care in an urban area. AIDS and Behavior, 14, 459-468. doi: 10.1007/s10461-009-9628-9
The chapter in this book explores the argument that partner notification should not be a mandated action when a person is found to be HIV positive. It discusses that it should be voluntary and confidential and that by making it mandatory, it may even deter people from getting tested for HIV at all. HIV is sometimes contracted by behavior that is illegal and there may be legal repercussions for getting tested. To give this information requires a degree of trust and cooperation and the populations that are most affected by HIV-gay men, minorities and intravenous drug users-are often already facing several barriers which include stigma, discrimination, lack of resources are most likely not inclined to not trust public health officials. Also even when given assistance to find partners, 66% could not be found (p 95). This article is important to examine how to reduce HIV infection because the argument is that this method is not efficient and effective. In fact, more damage could be done rather than reduce HIV infection. This information source is reliable in that it presents two sides of an argument. As its title suggests, it proposes opposing viewpoints on a subject, citing that it is a strength to understand one’s own argument when one knows the opponent’s. In comparison to other articles listed in this assignment, I have found that this is the first one that is clearly against this intervention as a method of reducing HIV spread. Kaliher, W. B. (2003). Partner notification should not be made mandatory. In T. L. Roleff (Ed.), AIDS: Opposing Viewpoints (pp. 88-97). Farmington Hills, MI: Greenhaven Press.
This article discusses how HIV/AIDS is a taboo topic in both an intimate relationship and in general. It stresses that it is misconceptions about how HIV is transmitted and managed creates a wide gap in identify HIV and treating it. If there is intimacy in a relationship, the topic should be broached but unequal power, inhibitions and sexual disorder can hinder this. This article goes on to explain how to conduct and interview with a patient and what approach to take so that the patients are more apt to opening up and be able to tell their story. This article in comparison to the others takes that standpoint of trying to get HIV out of the umbrella of silence and shame. Also, it looks to increase intimacy in relationships, something that can be lacking in a relationship with or with the presence of HIV. By increasing intimacy, HIV is more likely to be discussed. The article is from a reliable resource, but does have a bias in that females need to regain their locus of control. Often these women are victims to macho social conditioning. Although women of color are also heavily affected by HIV, this approach maybe a bit narrow for the other populations in the Metro Detroit area. Phil, K., B, D., & R, P. (2006). Intimacy and HIV. South African Family Practice, 48(2), 54-55.
This article discusses how most that are infected by HIV also have concurrent health problems, namely substance abuse problems and mental illness. As a result, there are multiple places where patients must go to get all of these needs met which can lead to failure of adhering to a medical regime or failure to get help needed. Many of these patients have barriers to care and it is not unusual to have someone who is being treated for substance use be excluded from mental health care (if drugs are being used for instance) or HIV care. By having integrated care and additional services that address basic needs (housing, transportation for example), HIV can be more successfully managed as patients can get a multitude of their needs met in one place. This article is reliable but does not present any measures or results of a direct study. Rather it proposes how this approach can be used to increase the success of helping prevent and manage HIV. This article has not changed how I think about my topic. If anything it really lays out a foundation as to how to decrease HIV infection by trying to address the barriers that people face to getting care in one place. Kuehn, B. M. (2008, August 6). Integrated care needed for patients with HIV, drug abuse, and mental illness. Journal of the American Medical Association, 300(5). doi: 10.1001/jama.300.5.494
This article focuses on a Detroit resident, Hank Milbourne, who is HIV positive and is a part of one of the populations most affected by HIV as an older gay black male. He is actively involved in the fight against AIDS. He is involved with the AIDS community, runs prevention programs, writes grants to help fund these programs and also serves as a mentor for many younger gay males. He strives to make AIDS a more open and upfront conversation and strives to make it a topic that can talked about in the community, stating that if AIDS is not talked about then it can’t be fought. Milbourne acknowledges that HIV has a strong prevalence in Detroit but because of the stigma associated with being HIV positive and gay, talking about it is not only challenging but also dangerous. This article is useful in that it is light and speaks about the prevalence of HIV in the area without being loaded with too many statistics and generally get the point across. By incorporating a citizen of Detroit who is HIV positive also gives it a human interest perspective. The source is biased in that it does state that Milbourne has “more courage in his little finger than most politicians or community leaders have in their entire bodies.” The article is not specific in stating that these politicians are from Detroit but does comment that Detroit would be able to better control HIV if politicians and community leaders followed Milbourne’s lead. This has not changed about how I think about this topic. Leaders can’t stay silent in the AIDS fight. (2010, August 8). Detroit Free Press. Retrieved from www.freep.com
This article explored the identification of interventions that demonstrated the best evidence of efficacy for reducing HIV risk. A cumulative database was developed and the efficacy criteria was based on several aspects of the a study. Quality of the study design, quality of implementation and analysis, and strength of evidence. The best evidence interventions that were determined in the study relied on at least one behavioral change model, the most common being Social Cognitive Theory. This article is a useful source because it displays what interventions have been found to be effective despite having different content, format, duration and target population. This article is reliable in that it also addresses its limitations in its review of interventions and suggests that this should be explored in the future. Another aspect that it did not explore was cost effectiveness. This article can be used as a guide as to how implement a model that can reduce HIV infection but whether or not it can be implemented with a realistic or real world budget remains to be in question. Lyles, C. M., Kay, L. S., Crepaz, N., Herbst, J. H., Passin, W. F., Kim, A. S., ... Mullins, M. M. (2007). Best-evidence interventions: Findings from a systematic review of HIV behavioral interventions for US populations at high risk, 2000-2004. American Journal of Public Health, 97(1). Retrieved from http://www.ncbi.nlm.nih.gov.proxy.lib.wayne.edu/pmc/articles/PMC1716236/pdf/0970133.pdf
This is a report that reviewed HIV/AIDS in Michigan. It looks at the state as a whole, the Metro Detroit Area and the rest of the state outside of Metro Detroit. HIV infection is spread disproportionately throughout the state. Although the Metro area comprises 44% of the state’s population, two-thirds of people who are HIV positive live there. Black males and females still continue to have the highest rate of infection compared to other races. There is also a significant increase in teens ages 13-19. Another population that is seen to have a increase is men who have sex with men (MSM). This report is current and comprehensive and specific to the epidemic of HIV/AIDS in Michigan and is a reliable source of information. It gathers its information from various reputable sources, both for its core HIV/AIDS knowledge and supplemental. It takes past studies and displays tables and graphs that represent the prevalence of HIV in the Metro Detroit Area. This source is helpful and useful to helping support that HIV infection is a serious problem in Metro Detroit especially with the increased numbers of those infected are teens. This sources also makes a point to list its strengths and limitations of the document as a whole and that although it may not represent the complete picture, it attempts to do so as much as possible. Michigan Department of Community Mental Health. (2010). 2010 Epidemiologic Profile of HIV/AIDS in Michigan (Annual Report). Retrieved from Epidemiological Profile of HIV/AIDS in Michigan website: http://www.michigan.gov/mdch/statisticsreports/communicable_diseases/hivaids/epidemiologic+profiles+of+hivaids+in+michigan
This article looks at addressing risky sexual behavior in youths with HIV to help prevent the spread of HIV and minimize physical consequences with being HIV positive. High sexual activity is considered to be the main way of transmission in people under the age of 25 and this age group is more likely to engage in high risk sexual behavior. This article fits well into prevention of HIV infection. The article discusses the use of the Transtheoretical Model which can be used not only for condom use but for substance use behavior as well. This model describes five stages of change that can help a person modify and maintain a change in behavior. This model is especially important since it can be used with people who have little to no motivation to change. The study performed in the article was small and mainly consisted to questionnaires to measure high risk sexual behavior, the subjects’ self-efficacy, social support, substance use, emotional distress and what stage of change the subjects were in. The goal of this article’s study was to provide a framework for understanding youths and to guide future intervention work. The study found that general social support and emotional distress may contribute to a better quality of life for a subject but did not have any effect on condom use. This article is from a peer reviewed journal and is reliable. It was not very broad in its scope but it is useful in the sense that it can help guide future interventions and what to focus on. Naar-King, S., Wright, K., Parsons, J. T., Frey, M., Templin, T., & Ondersma, S. (2006). Transtheoretical model and condom use in HIV-positive youths. Health Psychology, 25(5), 648-652.
This article looks at using the Transtheoretical model once more but this time targeting adherence to HIV treatment in youths. The intervention used is Motivational Interviewing, a patient centered, rolling with resistance means of communication to elicit change talk and strengthen any inner motivation for change. This article going into more depth about MI and its success with adult populations into antiretroviral medication. The article also mentions that although it has been recommended to use MI for adolescents, few studies have been conducted to address medicine adherence. The primary outcome for the study was a lower viral load for the subjects. The subjects received 4 sessions of MI intervention over 10 weeks. In conclusion, there was a significant reduction in viral load but it was not the optimal reduction which is for it to be undetectable. Also the differences were no longer significant after 9 months. This article implies that more intensive interventions or that more frequent brief interventions might be needed. This article is important to helping reduce HIV infection because although MI is effective, it may only do so temporarily if it is too short of a time. This study looked at a small sample from a specific age group. Naar-King, S., Parsons, J. T., Murphy, D. A., Chen, X., Harris, R., & Belzer, M. E. (2009, December). Improving heath outcomes for youth living with the human immunodeficiency virus. Archives of Pediatrics & Adolescent Medicine, 163(12). Retrieved from www.archpediatrics.com
This article discusses using rapid assessment to help address HIV in racial and ethnic minority cultures. This method relies on ethnographic and qualitative data collection and analysis to help bridge the gap between research that is program specific and gathering information about the environment, thus finding what interventions would be most effective. This article is important because it uses a strategy not often used in research. It was found that HIV prevention and care were available and widespread among communities but that often they were only available at times when those who were at most risk were active. This method of research can be used to fill the gaps in HIV outreach attempts. What is missing? What are we doing wrong? This article revealed that information that is given about HIV can still be misconstrued by local cultural beliefs and form a formidable barrier to HIV prevention. This resources is helpful because it can help us change take on a more adaptive approach to the community that is the target of outreach. Needle, R. H., Trotter, R. T., Singer, M., Bates, C., Page, B., Metzger, D., & Marcelin, L. H. (2003, June 2003). Rapid assessment of the HIV/AIDS crisis in racial and ethnic minority communities: An approach for timely community interventions. American Journal of Public Health, 93(6).
This article discusses the use of motivational interviewing with young African American males who have sex with men. This group is considered to be among the highest risk for HIV infection. According to additional tests mentioned in the article, they are a group that is also less likely to be tested for HIV and yet most likely to test positive for it in comparison to whites and Hispanics. This article continues to encourage the use of Motivational Interviewing as a method of intervention with this population due to their unawareness of their status. This article reported that those who received MI were more likely to return for their test results. This article’s test setting took place in Detroit, the specific urban area in crisis. Getting tested and finding out one’s status is the one of the first steps HIV positive people must make. Although this article and its study seems to be unremarkable in comparison, it shows consistency that Motivational Interviewing is an effective way to elicit change talk in clients. Outlaw, A. Y., Naar-King, S., Parsons, J. T., Green-Jones, M., Janisse, H., & Secord, E. (2010). Using motivational interviewing in HIV field outreach with young African American men who have sex with men: A randomized clinical trial . American Journal of Public Health, 100.
This article looks at how well internal medicine residents are trained in assessing patients for HIV either by means of testing, counseling and initial management of HIV. Although many of the residents reported that to it would be an excellent opportunity and many have planned to work with HIV patients, 39% reported that they did not feel competent to provide HIV care. Residency training in HIV care remains largely inpatient based and residents frequently rate that of outpatient as inadequate. This article was useful in that there is a potential gap for HIV to not be detected in an outpatient setting. Compared to other sources, this mostly looks at improving ambulatory care for patients who have HIV. This source is reliable but does have its limitations and acknowledges that being that the information was collected by self report and thus subject to recollection bias. This source was helpful in showing that HIV care is not as prominent in residency curricula and it is important that doctors of the future learn how to address high risk patients. In order for HIV prevention to be best executed, it must include prevention from many points. This would also include what doctors can do when the patient is present. This article has not changed how I think about HIV prevention. Phillips, K. A., Cofrancesco, J., Sisson, S., Wu, A. W., Bass, E. B., & Berkenbilt, G. (2010). A multicenter study of internal medicine residents’ perceptions of training, competence, and performance in outpatient HIV care. AIDS Patient Care and STDs, 24(3).
This article looks at the cost of using rapid testing to identify people who are HIV positive in an outreach setting. Often people who are HIV positive do not know it and because they are unaware of their status, they are at risk for transmitting it to others. Conventional testing requires that patients come back to the clinic for their results should they get tested which takes about one to two weeks. Not all patients return. This article looks at offering rapid testing at a free health clinic and in outreach settings. The cost of providing rapid testing in an outreach setting was found to be considerably higher than in the clinic. This article is important because it shows that to provide outreach to diagnose and possibly prevent HIV in an outreach setting is going to be more costly yet outreach is such a critical piece in trying helping people get into care. Often people would not come into a clinic for testing on their own. This article does have limitations and admits that there could be error in recalling all the costs. It concludes that outreach settings pilot test rapid testing before investing money in a similar project. Shrestha, R. K., Clark, H. A., Sansom, S. L., Song, B., Buckendahl, H., Calhoun, C. B., ... Heffelfinger, J. D. (2008). Cost-effectiveness of finding new HIV diagnoses using rapid HIV testing in community-based organizations (123). Retrieved from http://www.publichealthreports.org: http://www.publichealthreports.org/archives/issueopen.cfm?articleID=2139
This article does not directly address HIV but the techniques described here are useful in being able to helping elicit change talk in patients and helping them find their own inner motivations for change. The unique blending of both motivational interviewing and ethnographic interviewing to help patients remain or continue in mental health care. It is with racial and ethnic minority groups that are most likely to dropout or have poor attendance in mental health care. These techniques are more culturally sensitive and competent which is important as there is already a mistrust that these populations have of these services. Since the majority of those who are affected by HIV are minorities, these methods may help be successful in reducing HIV infection. This article is reliable and appears to have no bias. It has not changed the way I think about my topic and in comparison to other articles, it is very detailed and specific about the use of just one additional engagement session to treatment and how it was met with reasonable success in keeping a patient in treatment. Swartz, H. A., Zuckoff, A., Grote, N. K., Spielvogle, H. N., Bledsoe, S., Shear, M. K., & Frank, E. (2007). Engaging depressed patients in psychotherapy: Integrating techniques from motivational interviewing and ethnographic interviewing to improve treatment participation. Professional Psychology: Research and Practice, 38(4), 430-439. doi: 10.1037/0735-7028.38.4.430
This government document outlines 3 goals for addressing HIV in the United States: 1.) Reduce new HIV infections 2.) Increasing access to care and improving health outcomes for people living with HIV and 3.) reducing HIV-related health disparities. It states that HIV prevention efforts need to be intensified in communities where HIV is most heavily concentrated. This would include the Detroit area. It stressed the need to make it a coordinated effort on all government levels, federal and state, to accomplish these goals. Although the strategy outlines ideas and plans to reach these goals, it admits that it is not a budgetary report and that the strategies that are outlined here should be used to take current efforts and focus on better delivery with existing funds. It draws heavily on targeting communities that are most affected by HIV, making interventions population specific although any population could be susceptible to contracting HIV. Concentration on these specific populations may continue the stigma that HIV carries and link it to these populations. This document has not changed my viewpoint on HIV prevention so much as introduce new ideas. There is no one sole effective prevention for preventing the spread of HIV and therefore it is important that all points of both prevention and interventions be looked at. The White House Office of National AIDS Policy. (2010). National HIV/AIDS strategy for the United States. Retrieved from White House website: www.whitehouse.gov.onap