Download
1 / 25
350 likes | 826 Views
EOSINOPHILIC ESOPHAGITIS. ATILLA ERTAN, MD, FACP, AGAF, MACG. Disclamer. Grant/Research Support from Centocor, Abbott Labs, Elan-Biogen, UCB Salix &Sucampo Pharmaceuticals, Genentech, Axcan & Barrx Inc.

E N D
EOSINOPHILIC ESOPHAGITIS ATILLA ERTAN, MD, FACP, AGAF, MACG
Disclamer • Grant/Research Support from Centocor, Abbott Labs, Elan-Biogen, UCB Salix &Sucampo Pharmaceuticals, Genentech, Axcan & Barrx Inc. • Scientific Advisory Board Member for Centocor, UCB Pharmaceuticals Inc, Abbott Laboratories & Prometheus Labs.
Learning Objectives for EoE • Recognize & differential diagnosis • Understand its pathogenesis • Identify diagnostic criteria • Recognize management difficulties & different therapeutic approaches
Eosinophilic Esophagitis (EoE) • 12 adults over 2 yr period with >20 IEE • Dysphagia predominant complaint • Unremarkable EGD • pH monitoring normal in 11 Attwood SE et al, Dig Dis Sci 38; 109, 1993
D.W.S.# 1740111-8 A 37 y/o male with a 5 yrs h/o intermittent food dysphagia & food impactions who had related ER visits. During one of these episodes, he came to TMH ER. MED: None ALL: Penn, shellfish PMH/PSH: Hay fever SH: Married, lawyer, denied T, ETOH & IVDA FH: Noncontributory ROS/PE: Unremarkable Emergent EGD & biopsy findings
D.W.S. # 1740111-8 Post food impaction 3-20-2003 Food impaction 3-20-2003
D.W.S. # 1740111-8Linear furrowing, vertical lines & white specks
EOSINOPHILIC ESOPHAGITIS [EoE] EoE is a chronic and recurrent inflammatory disease with increase prevalence woldwide and characterized by; Dysphagia, food impaction, GERD & less commonly chest pain in predominantly white males (75-82%) ≥15 intraepithelial eosinophils/HPF leads to fibrosis and angiogenesis, with mural thickening, loss of elasticity of the esophageal wall and stricture formation. Exclusion of other disorders associated with similar clinical, histological, or endoscopic features ____________________________________________ Gastroenterol 133: 1342-63, 2007, Gastroenterol 134: 204-14, 2008 & Gastroenterol 140: 82-90, 2011.
PATHOGENESIS OF EoE • EoE is associated with an allergic response to environmental antigens that lead to cytokine mediators associated esophageal eosinophilia. • IL-5, IL-13 , IL-15 and other cytokines may play a major role in eosinophilic recruitment by response to certain food proteins. • There is a clear disarray between circular & longitudinal muscle contractions during the peristalsis. • Esophageal distansibility was significantly reduced compared with controls by using a functional luminal imaging probe [EndoFLIP]. ______________________________________________________________________________________________________________________________ J Allergy ClinImmunol 120: 1292-300, 2007 Gut 59: 12-20, 2010 Gastroentrol 138: 275-284, 2010; 139: 182, 2010; 140: 82-90,2011
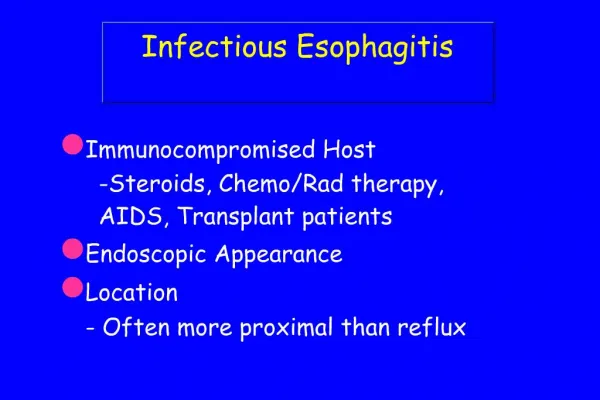
ENDOSCOPIC FEATURES OF EoE ______________________________________ • Unremarkable endoscopic mucosa & lumen. • Circular rings, transient or fixed, “feline esophagus” • Linear furrowing, vertical lines of the mucosa • Linear shearing/”crepe paper” mucosa with passage of endoscope or dilator • White exudates/specks, nodules or granularity • Stricture/rings: proximal, middle, or distal. ______________________________________ Gastroenterol, 133: 1342, 2007 (modified). * None of the features are specific for EoE.
I.E. # 3659813-1Barrett’s islands & EoE with transient circular rings
EGD biopsy for patients with EoE • More than 5-6 biopsies had a sensitivity of 100% even in an unremarkable mucosa. • Due to scaterred histologic distribution, proximal, mid & distal esophagus should be biopsied. • Mucosal eosinophilia may show a seasonal variation, possibly related to allergies. Gastrointest Endosc, 64; 313, 2006 Am J Gastroenterol, 104; 716, 2009 ;
Differential Diagnosis of EoE _______________________________________ Crohn’s disease* Connective tissue disorders* Hypereosinophilic syndrome Infections [herpes & candida]* Drug sensitivity response Eosinophilic gastroenteritis _______________________________________ *These diseases may have intraepithelial eosinophilia but less than 15/HPF in one or more biopsy specimens.
EoE & BARRETT’S ESOPHAGUS [BE] • “BE or BD has not been reported in patients with EoE” (1,2). • “EoE is not a disease characterized by mucosal ulceration or destruction. Therefore, it seems likely that the pathologic process of EoE is different from that of GERD and that adenoca or squamous ca of the esophagus are not the spectrum of EoE” (2). Recent studies and our experience showed that this relation is not uncommon. 1. Am J Gastroenterol, 101: 1900, 2006. 2. Gastroenterology, 133: 1342, 2007.
A.P.# 01911497-4 A 47 y/o male with a 9-10 yrs h/o GERD who had recent dysphagia & few episodes of food impaction. He diagnosed as having L.S. Barrett’s with HGD/LGD & EoE. MED: Zegerid 40 mg BID PMH/PSH & FH: Unremarkable. SH: Married, IT executive, no tobacco, ETOH or IVDA. ROS: Gained 40 lbs within last 10 yrs. PE: Essentially unremarkable except moderate obesity. LAB: Unremarkable CBC-diff, SMA-6 & other blood tests. Chest/abd CT scan EUS
Case AP Previous history of food impactions:
A.P. #01911497-4L.S. BE with MF/HGD & EoE with transient circular rings
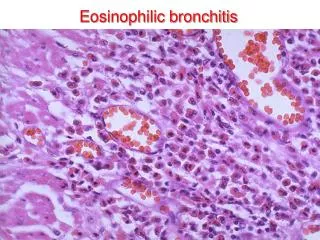
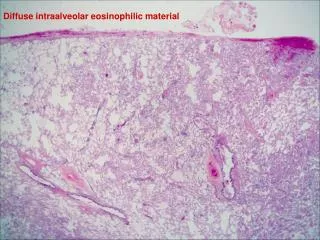
Case AP Pathology Basal zone hyperplasia, increased eosinophils Intraepithelial eosinophils of eosinophils
ALLERGY EVALUATION IN PATIENTS WITH EoE • The majority of patients with EoE is atopic based on the coexistence of atophic dermatitis, allergic rhinitis, and/or bronchial asthma with + antigen skin sensitization & abnormal plasma antigen-specific IgE. • 10%-50% of adults had peripheral eosinophilia. • Most patients improve on allergen-free diets. • Allergist consultation may be recommended. __________________________________________________________ ClinGastroenterolHepatol 3:1198-206, 2005. J PediatrGastroenterolNutr 42:22-6, 2006.
Medical Management # 1 • Removal of allergenic foods [diary, eggs, wheat, soy, peanuts, fish/shellfish]- with unpredictive allergy testing in adults-, may be effective. The elemental diet may be helpful in severe cases (1) • Endoscopic dilatation is useful in pts with fixed strictures/rings. The risk of mucosal tearing and perforation are relatively higher (2,3). _____________________________________________________________________ 1. ClinGastroenterolHepatol 4: 1097-102, 2006. 2 & 3. Gastroenterology 127: 364-5, 2004; 133:1342-6, 2007.
MEDICAL MANAGEMENT # 2 • 16 to 50% of pts showed improvement with PPI treatment (1,2) • Topical [rarely systemic] corticosteroids resolve symptoms. Fluticasone 440 mcg BID for 6-8 weeks may be effective for an induction therapy (3) • A pilot trials with anti-IL-5[Mepolizumab], leukotriene D4 receptor ab [Montelukast] & Infliximab showed improvement in pts with severe EoE. • Budesonide suspension (0.25 mg/ml) inhalation BID (4) for 50-wks. ___________________________________________________ 1 & 2. J Gastroenterol 101: 1666-70, 2006 & ClinGastroenterolHepatol 9: 110-7, 2011 3. GastrointestEndosc 63:3-12, 2006 ClinGastroenterolHepatol 9: 400-9, 2011