Download
1 / 68
850 likes | 1.77k Views
Overview of Eosinophilic Esophagitis. Gabriel Rendon, M.D. Texas Digestive Disease Consultants. Case Vignette. CC: Dysphagia

E N D
Overview of Eosinophilic Esophagitis Gabriel Rendon, M.D. Texas Digestive Disease Consultants
Case Vignette • CC: Dysphagia • HPI: 28 year old white man referred to the GI clinic with three years of dysphagia. Intermittent, non-progressive, worse with solids; He also noted occasional sub-sternal chest pain. Denied heartburn, abdominal pain, weight loss, or change in bowel habits. Trial of Nexium was not helpful.
HPI (cont) • PMH: Allergic rhinitis • Meds: Allegra, Nexium • NKDA • SH: Nonsmoker, rare EtoH use, no drug use. • FH: No significant GI diseases.
Physical Exam • Vital signs: T 98.8 HR 86 BP 126/76 RR 16 • GEN: WNWD, NAD; • HEENT: normal; • CHEST: CTA; • CV: RRR no M/R/G; • ABD: S, NABS, NT, ND; • EXT: normal;
LABS • CBC: WBC 8.0 Hgb 14.6 PLT 288 • 68 PMN 18 L 10 E 3 Mo • Chem: WNL • LFT’s: • AST 26 ALT 22 AlkPho 80 TB 0.6 DB 0.2
Endoscopy Distal esophagus Mid esophagus
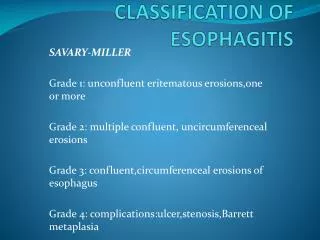
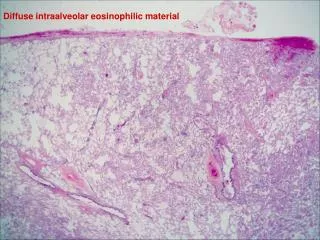
Pathology Report: “Squamous mucosa with erosion, basal hyperplasia, increased papillae height, intercellular edema, and over 60 eosinophils per HPF. This is consistent with eosinophilic esophagitis.”
Eosinophilic Esophagitis • Inflammatory disorder of the esophagus characterized by accumulation of eosinophils in the epithelium and a range of symptoms • First reported in the 1978 • Prior to 1995, there were only 12 manuscripts about EoE • More than 250 articles written in the past 10 years
Definition1 • A clinicopathologic disorder of the esophagus characterized by a dense esophageal eosinophilia (>=15 eos/HPF) with severe squamous hyperplasia and upper GI symptoms • Gastric and duodenal biopsies are normal • No response to PPI therapy or normal pH monitoring 1. Furuta, et al. Eosinophilic Esophagitis in Children and Adults: A systematic review and Consensus recommendations for Diagnosis and Treatment. Gastroenterology 2007; 133: 1342-1363.
Pathogenesis • Still poorly understood • The cellular and cytokine milieu similar to bronchial asthma [8] • Food allergens and/or aeroallergens • Recent study of 19 pts observed documented food and aero-allergies in 18/19 (94.8%) [30] • seasonality and association with pollen count has been demonstrated [3] • Evidence of disease remission in children fed an elemental diet [31]
Pathogenesis (cont) • Association/Overlap with GERD • Eosinophil derived inflammatory proteins (Il-6, PAF’s, vasoactive peptides) induce LES relaxations and decreased esophageal contractions [32] • Acid/pepsin can damage tight junctions-> increased permeability->antigen exposure to deeper layers [33] • Some cases of “classic” EoE have responded to dramatically to PPI’s [34]
Epidemiology • Males affected more commonly than females1 • Adults: 76% male, mean age 38 • Can affect all races and ethnicities • In Olmsted county, prevalence 55/100,000 ( 0.05%) [35] • Recent systematic review of 9 papers [36]: • Population based prevalence of .03% • Symptom based prevalence of 2.8%
Prevalence in Selected Populations • Solid Food dysphagia • Prasad27 prospectively studied 222 patients undergoing endoscopy with biopsy for solid food dysphagia; Overall 33/222 (15%) had EE • Mackenzie et al29 prospectively studied 94 pts presenting with dysphagia: 11/94 (11.7%) met histologic criteria for EE • Food impaction • Desai et al5 reported 31 patients presenting with food impaction over a 3 year period 17/31 (54%) had histology consistent with EE
Clinical Features • Children • Feeding intolerance • Failure to Thrive • Heartburn • Emesis • Dysphagia/Food impaction • Refractory GERD • Adults • Intermittent dysphagia • Food impaction • Chest pain • Refractory GERD
Symptoms • Straumann8 prospectively re-examined 30 patients with known EoE • 30/30 (100%) intermittent dysphagia with food impactions • 2/30 (6.7%) Heartburn • Croese6 reviewed 31 patients with EoE in Australia • 27/29 (93%) Dysphagia • 19/27 (70%) Food Impactions • 13/27 (48%) Heartburn • 13/27 (48%) Chest Pain • 1/27 (3.7%) Abdominal pain • Symptoms fluctuated over time; long symptom free intervals 6.Croese et al. Clinical and endoscopic features of eosinophilic esophagitis in adults. Gastrointestinal endosc 2003;58:516-22. 8. Straumann et al. Eosinophilic esophagitis: red on microscopy, white on endoscopy. Digestion 2004;70:109–116.
Symptoms (cont) • Kaplan4 reviewed 8 cases of EoE over 10 year period • 8/8 (100%) has dysphagia • Potter13 retrospectively reviewed 29 patients with EoE • 24/29 (83%) had dysphagia • 8/29 (28%) had food impaction • 9/29 (31%) had refractory GERD • Remedios9 prospectively studied 26 patients with EoE • 26/26 (100%) reported dysphagia • 17/26 (65%) reported food impaction • 17/26 (65%) were previously dx with GERD • 2/26 (7.6%) reported chest pain • Kaplan et al. Endoscopy in eosinophilic esophagitis. Clinical gastroenterology and hepatology 2003;1:433– 437. • 9 . Remedios et al. Eosinophilic esophagitis in adults: clinical, endoscopic, histologic findings, and response to treatment with fluticasone propionate. Gastrointestinal Endosc 2006;63:3-12. • 13. Potter et al. Eosinophilic esophagitis in adults: an emerging problem with unique esophageal features. Gastrointestinal endosc 2004;59:355-61
Natural History • Straumann et al3 (2003) prospectically studied 30 adults with EoE • Mean follow up 7.2 years (1.4-11.5) • Dysphagia • 7/30 (23.3%) reported increasing • 11/30 (36.7%)reported stable persisting • 11/30 (36.7%)improving • 1/30 (3.4%) asymptomatic 3. Straumann, et al. Natural history of primary eosinophilic esophagitis. Gastroenterology 2003; 125:1660-69.
Natural History (cont) • BMI and nutritional status maintained • Endoscopic findings remained stable • Laboratory values remained stable (peripheral eosinophilia, IgE, albumin) • Histology improved over time • 6/7 subjects with subepithelial tissue sampling had significant fibrosis and sclerosis • Response to therapy • 11/30 underwent dilation • 10/11 responded well
Endoscopy • Endoscopic findings can be subtle • Linear furrowing • Ringed or corrugated (trachealization or felinization) • White exudates, specks or nodules • Linear shearing/crepe paper mucosa • Stricture • Small caliber esophagus • Solitary ring • Normal
Endoscopy • Desai et al5 identified 17/31 (54%) presenting with food impaction with histology consistent with EoE • 17/17 (100%) had rings and furrows • 5/17 (29%) strictures (4 proximal, 1 distal) • Croese et al6 retrospectively reviewed 31 patients diagnosed with EoE • 30/31 (97%) had furrows (with or without rings) • 17/31 (54%) had strictures 5. Desai et al. Association of eosinophilic inflammation with esophageal food impaction in adults. Gastrointestinal endoscopy 2005; 61: 795-801.
Endoscopy • Straumann et al8 retrospectively reviewed 30 adult patients with EoE • 16/30 (53%) had white exudates • 13/30 nodules • 12/30 plaques • 15/30 (50%) had concentric rings • 13/30 (43%) had stricture • 11/30 (38%) had a solitary ring • 4/30 (13%) had crepe paper mucosa • Straumann et al7 reported a series of 5 patients with EoE and mucosal friability • 5/5 (100%) had “crepe-paper mucosa” leading to lacerations • Postulated that mucosal fragility is pathognomonic for EoE 7. Straumann et al. Fragility of the esophageal mucosa: A pathognomonic endoscopic sign of primary eosinophilic esophagitis? Gastrointestinal endosc 2003; 59: 407-412.
Straumann et al8 8. Straumann et al. Eosinophilic esophagitis: red on microscopy, white on endoscopy. Digestion 2004;70:109–116.
Endoscopy • Remedios et al9 prospectically enrolled 26 patients with histopathologic EoE (>15 eos/HPF) • 20/26 (77%) had linear furrows • 16/26 (61%) had mucosal rings • 7/26 (27%) had narrow esophagus • 4/26 (15%) had white papules/plaques
Biopsy Procurement • Gonsalves et al10 reviewed 66 patients (341 specimens) with EoE • Number of biopsies needed varied with threshold • >15 eos/HPF: 5 biopsies had sensitivity 100% • 1 biopsy had sensitivity of 55% • >30 eos/HPF: 5 biopsies had sensitivity 89% • 20 patients had biopsies from both proximal and distal sites • Mean 68 eos/HPF proximally, 82 eos/HPF distally (NS) • 16/20 patients had distal eosinophilia and no proximal eosinophilia • Remedios reported 1 patient with proximal eosinophilia (25 eos/HPF) and no distal eosinophilia 10. Gonsalves et al. Histopathologic variability and endoscopic correlates in adults with eosinophilic esophagitis. Gastrointestinal Endosc 2006;64:313-9.
Radiology • Upper GI contrast studies may demonstrate strictures, rings, corrugations • May show small caliber esophagus not readily appreciated by endoscopy • Zimmerman et al10 reviewed 14 pts with EoE • 10/14 had strictures • Mean length of 5.1 cm • 7/10 had concentric rings along the stricture 10. Zimmeman et al. Idiopathic eosinophilic esophagitis in adults. Radiology 2005; 236:159 –165 .
Histology • Historically, esophageal eosinophilia thought secondary (pathognomonic) to GERD1 • 1995, Kelly et al14 described 10 children with GERD type symptoms, intense esophageal eosinophilia and no response to acid suppressive therapy • Several more studies described patients with refractory GERD symptoms and eosinophilia1 • In GERD, eosinophilia is mild, usually <10 eos/HPF and confined to distal esophagus • In EoE, the eosinophilia is more intense, >15 eos/HPF (often much greater) and throughout the esophagus 14. Kelly KJ et al. Eosinophilic esophagitis attributed to gastroesophageal reflux: improvement with an amino acid-based formula. Gastroenterology 1995;109:1503–1512.
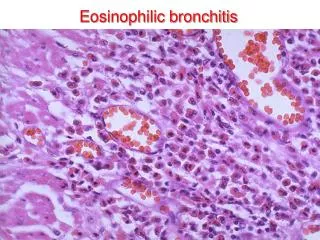
Histology Features • Markedly increased intraepithelial eosinophils • Superficial layering • Basal zone/papillary hyperplasia • Eosinophilic micro-abscesses • Degranulation (MBP) • Edema • Other cells (Lymphocytes, PMN, Mast cells) • Subepithelial fibrosis
Histologic Features • Gonsalves10 studied 66 patients with 341 biopsy specimens • Median count was 107 eos/HPF (0-557) • 93% Epithelial hyperplasia • 90% Superficial layering • 75% eosinophilic microabscess • 52% degranulation
Histologic Features • Straumann et al (peak method) • Mean count in proximal esophagus was 78 eos/HPF • Mean count in distal esophagus was 117 eos/HPF • Papillary hyperplasia was seen in 80% • Basal zone hyperplasia was seen in 65% • Remedios et al (mean method) • Mean count in proximal esophagus was 25 • Mean count in distal esophagus was 39
Histology • Parfitt15 studied biopsied from 41 pts with EE (>15 eos/HPF x2) and 116 pts with GERD: 15. Parfitt et al. Eosinophilic esophagitis in adults: distinguishing features from gastroesophageal reflux disease: a study of 41 patients. Modern pathology (2006) 19, 90–96.
History of Allergy or Atopy • Remedios9 et al reviewed 26 pt with EoE • 20/26 (77%) patients had an atopic history (Asthma, hay fever, rhinitis, food allergy or atopic dermatitis) • Straumann et al11 • 18/30 (60%) had history of atopy • Croese et al6 • 28/30 (93%) had an allergic history
Peripheral Eosinophilia • Peripheral eosinophilia associated with atopic conditions • Problematic in that there was a difference in thresholds • Straumann3 reported 12/24 (50%) with mild elevation (350-1500 cells/mm3) • Parfitt15 reported 1/10 (10%) with >800 cells/mm3
Atopic/Allergy Testing Skin prick test and atopic patch test have been used in children in 2 published studies17,18 • Resolution of symptoms and histology in 77% with elimination diet in identified allergens • Elemental diets effective in the rest • Recent study of 19 adult pts observed documented food and aero-allergies in 18/19 (94.8%) [30] • Spergel Et Al. Treatment Of Eosinophilic Esophagitis With Specific Food Elimination Diet Directed By A Combination Of Skin Prick And Patch Tests. Ann Allergy Asthma Immunol 2005;95:336 –343. • Spergel Jm, Beausoleil Jl, Mascarenhas M, Et Al. The Use Of Skin Prick Tests And Patch Tests To Identify Causative Foods In Eosinophilic Esophagitis. J Allergy Clin Immunol 2002;109:363–368.
Treatment • PPI • Topical steroids • Endoscopic dilation • LT receptor antagonists and mast cell stabilizers • Dietary changes
PPI • Can be part of diagnosis • Lack of a clinicopathologic response in patients with esophageal eosinophilia virtually diagnostic of EoE • Can be used in lieu of 24 hr pH monitoring1 • Concomitant therapy • Remedios9 showed pts with EE, 10/26 had abnormal 24 hr pH probes • Recent study in press reported 75% (26/35) response rate in unselected patients with eosinophilic infiltration
Topical Steroids • First reported use in 19981 • Arora22 identified 21 patients with EoE and treated them with swallowed FP 220 ug bid x6 weeks • All had resolution of their solid food dysphagia • Rapid relief within several days • Recurrences occurred 12-18 months later • Histology was not assessed • No oral candidiasis 22. Arora As, Perrault J, Smyrk Tc. Topical Corticosteroid Treatment Of Dysphagia Due To Eosinophilic Esophagitis In Adults. Mayo Clin Proc 2003;78:830 – 835
Remedios et al • 19/26 subjects were treated with swallowed FP 440 ug bid x 4 weeks • All 19 had symptom relief • 18/19 histologic improvement • Mean proximal eosinophil count decreased from 24.98 to 4.46 • Mean distal eosinophil count decreased from 39.3 to 3.8 • 3 patients developed asymptomatic esophageal candidiasis
Topical Steroids • Pediatric randomized double blind placebo controlled trial by Konikoff23 et al • 31 patients randomized to swallowed FP 440 bid x 3 months or placebo • 10/20 (50%) had histologic resolution in the FP group • 1/11 (9%) histologic resolution in placebo group (P =.047) • Recent randomized double blind placebo controlled trial of oral budesonide [37] • 13/18 resonse rate; 4/18 placebo • Mean eosinophil count 66->5