Download
1 / 26
310 likes | 1.26k Views
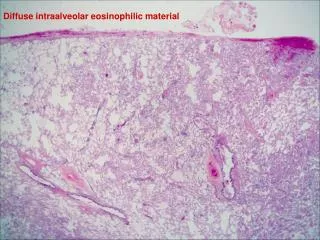
Eosinophilic bronchitis. Th2. Th2. Mast cell. Mast cell. IL-4. IL-5. Eosinophilic bronchitis. Late asthmatic reaction. Airway hyperresponsiveness. Exercise, cold air. Allergen. Early asthmatic reaction. Symptoms are nonspecific. Other respiratory and non-respiratory conditions.

E N D
Th2 Th2 Mast cell Mast cell IL-4 IL-5 Eosinophilic bronchitis Late asthmatic reaction Airway hyperresponsiveness Exercise, cold air Allergen Early asthmatic reaction
Symptoms are nonspecific Other respiratory and non-respiratory conditions Symptoms Variable airflow limitation Chronic airflow limitation Inflammation Airway hyperresponsiveness Hargreave F, AAAAI 2006
Induced sputum in OA: usefulness • To identify occupational eosinophilic bronchitis (due to an allergen or chemical sensitizer) with or without asthma. • This is done by serial measurements of induced sputum following periods at work and away from work. • Eosinophils that increase at work and fall away from work indicate eosinophilic bronchitis. • To support the diagnosis when the workplace sensitizer is unknown. • To monitor airway inflammation before/after specific inhalation challenge (SIC).
Induced sputum Compatible clinical history Work-relatedness • Asthma diagnosis • Reversible airflow obstruction • AHR • Sensitization • Skin prick tests • Sepecific IgE Methacholine test + – Return to work No longer at work Still at work SIC PEF monitoring SIC – + – + No Asthma Non-occupational asthma Occupacional asthma Chan-Yeung M, Malo JL. N Eng J Med 1995
Changes in induced sputum after specific inhalation challenges
Clinically significant increase: 0.26 x106 eosinophils/mL Lemière C et al. J Allergy Clin Immunol 2001;107:1063-8
After budesonide 800 mcg/day one month Latex 99 ng/m3 60 minutes Latex-induced eosinophilic bronchitis % Fall in FEV1 % eosinophils in sputum 120 80 100 60 80 60 40 40 20 20 0 0 bas 10 20 30 min 1h 2h 4h 6h 8h 10h 24h Allergen challenge PC20 > 16 mg/ml PC20methacholine > 16 mg/ml Quirce et al. JACI 2001
Normal Peak Expiratory Flow variability PEF L/min Days at work
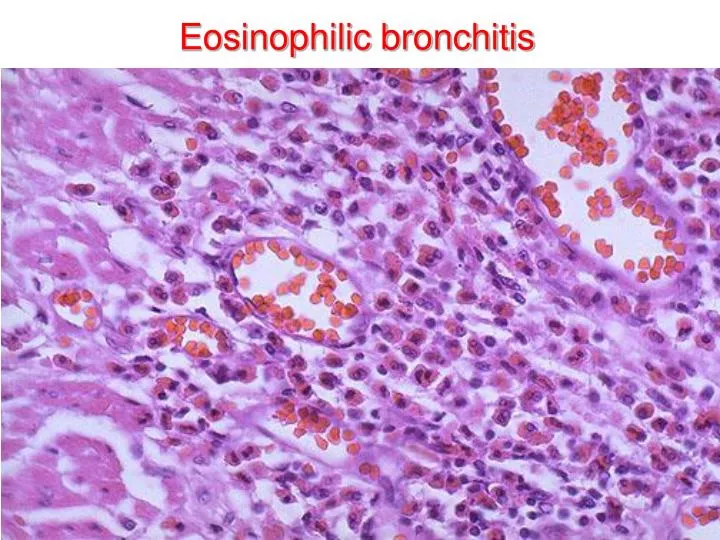
Eosinophilic bronchitis • Isolated chronic cough, productive of sputum • Normal lung function without variable airflow limitation • Airway hyperresponsiveness absent • Eosinophilia in sputum and BAL • Cough reflex to capsaicin increased • Normal daily variability in peak expiratory flow (<20%) • Upper airway symptoms are common • Middle age patients • Smoking is unusual • Prevalence of atopy similar to general population • Cough, sputum eosinophilia and cough reflex to capsaicin improve with inhaled corticosteroids Gibson et al. Lancet 1989
Causes of isolated chronic cough Brightling CE et al. AJRCCM 1999
Microlocalization of mast cells in the airway smooth muscle Brightling CE et al. N Eng J Med 2002
* * * * A C D B Sastre B et al (submitted).
† † * PGE2 LTC4 A B Sastre B et al (submitted).
Diagnostic criteria for occupational eosinophilic bronchitis • Isolated chronic cough (lasting more than 3 weeks) that worsens at work • Sputum eosinophilia 3% in sputum • Increases in sputum eosinophils are related to exposure to the offending agent (either at work or after SIC) • Spirometric parameters are normal and are not significantly affected by exposure to the offending agent • Absence of bronchial hyperresponsiveness to methacholine both at work and away from work • Other causes of chronic cough are rule out. Quirce S. Curr Opin Allergy Clin Immunol 2004;4:87-91
Remarks • The examination of induced sputum should be part of the diagnostic algorithm for workers who complain of asthma-like symptoms in the workplace. • Induced sputum is a diagnostic tool complementary to objective monitoring of lung function during periods at work and away from work, and before/after specific inhalation challenge • Eosinophilic bronchitis (without asthma) should be regarded as an occupationally-induced condition when work related changes in sputum samples are significant and reproducible.
Recommendations • In patients with chronic cough due to nonasthmatic eosinophilic bronchitis, • the possibility of an occupation-related cause needs to be considered. (Level of evidence, expert opinion; benefit, substantial; grade of recommendation, E/A) • when a causal allergen or occupational sensitizer is identified, avoidance is the best treatment. (Level of evidence, expert opinion; benefit, substantial; grade of recommendation, E/A) • first line treatment is inhaled corticosteroids (except when a causal allergen or sensitizer is identified). Level of evidence low; benefit, substantial; grade of recommendation, B. • If symptoms are persistently troublesome and/or the natural history of eosinophilic airway inflammation progresses despite treatment with high dose inhaled corticosteroids, oral corticosteroids should be given. (Level of evidence, expert opinion; benefit, substantial; grade of recommendation, E/A) Brightling CE. Chest 2006;129:116S-21S
Follow-up of patients with EB after treatment with ICS Park SW et al. Chest 2004
Observational study of the natural history of eosinophilic bronchitis • 52 patients with EB, 32 with follow-up 1 year • Mean duration of follow-up: 3.1 years (1-6 years) • 3 patients developed asthma (9%) • 5 patients FEV1/FVC (post-bd) <70% (16%) • 1 complete resolution of cough and eosinophilia (3%) • 13 persistent cough and eosinophilia >3% on one or more occasions (41%) • 7 persistent cough and eosinophilia < 3% (22%) • 3 symptom free and eosinophilia >3% occasionally (9%) Berry MA et al. Clin Exp Allergy 2005
Not all cases of occupational asthma are associated with airway eosinophilia, and airway inflammation with eosinophils may occur in the absence of asthma
Wardlaw AJ et al. Multidimensional phenotyping: towards a new taxonomy for airway disease.Clin Exp Allergy2005;35:1254-62.
Wardlaw AJ et al. Multidimensional phenotyping: towards a new taxonomy for airway disease.Clin Exp Allergy2005;35:1254-62.