Download
1 / 109

E N D
IMMUNE RESPONSE Dr.T.V.Rao MD Dr.T.V.Rao MD
Human Body is a Complex Structure Dr.T.V.Rao MD
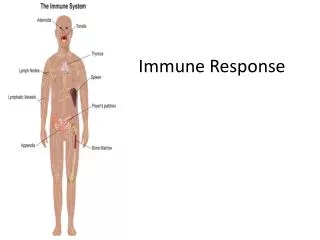
Immune System Controls the Immune Responses Dr.T.V.Rao MD
Organs of Immunity Coordinate different functions Dr.T.V.Rao MD
Immunity is a less Understood Puzzle Dr.T.V.Rao MD
Path of Immune Response Dr.T.V.Rao MD
Immune Response Protects Dr.T.V.Rao MD
11 Dr.T.V.Rao MD
Immune Response – A complex Mechanisms Dr.T.V.Rao MD
Several Cell Interaction compromises the Immune Response Dr.T.V.Rao MD
B Cells and T Cells work in Coordination Dr.T.V.Rao MD
Immune response works at Cellular level Dr.T.V.Rao MD
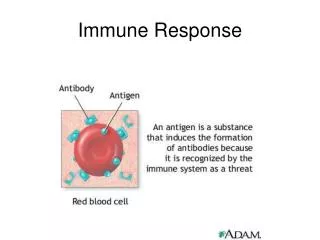
The Immune response An immune response is what the immune system does when confronted by an antigen. An immune response is an elaborate interplay between antigen, non-specific defenses, and B and T lymphocytes. The process involves direct contact (cells, molecules bind to receptors on cell surfaces) and cytokines (messenger molecules) that also bind to receptors on cell surfaces. 16 Dr.T.V.Rao MD
Results of Immune Response • Beneficial, • Indifferent, • Injurious, Reactions follow against any antigen either living or dead. May respond in Specific or No reactivity or Tolerance. Dr.T.V.Rao MD
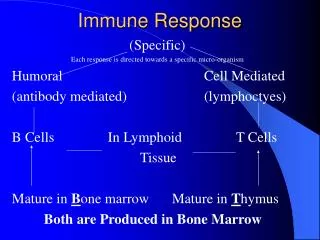
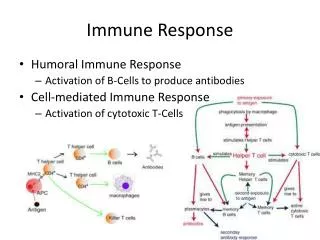
Classification of Immune Response 1 Humoral 2 Cell Mediated type • May work together. • May work in opposite way, • One may be more active than other. Dr.T.V.Rao MD
Active against Most Extra cellular Bacterial pathogens Viruses, Participates in Type 1 , 2, 3, Hypersensitivity reactions Auto Immune Disorders. Protects against, Fungus, Viruses IC bacterial infections Rejection of Homograft ,GVH, Immunological survelliance,cancer T cell mediated Hypersensitivity Auto Immune Disorders Immune ResponseHumoral / Cell Mediated Dr.T.V.Rao MD
Structure of Immunoglobulin Dr.T.V.Rao MD
Humoral Immune Response • Produces Antibodies B Cell – Plasma cell • Antigen Presented to Immunocompetent cells Processed – • Secretion of Antibodies, Dr.T.V.Rao MD
Production of Antibodies • Immune response is brought about by three types of cells • 1 APC macrophages, and dendritic cells, • 2 T Cell and 3 B cells • The first step is capture and processing of antigens by APC and their presentation with the association of appropriate MHC molecule to T cells • However some polysaccharides and simple molecules with repeating epitopes do not require T Cell participation Dr.T.V.Rao MD
Stages of Antibody mediated immune response • Contain three stages 1 The entry of antigen, its distribution and fate in the tissues and its contact with appropriate immunocompetent cells 2 The secretion of antigen by cells and the control of the antibody forming process 3 The secretion of antibody its distribution in tissues and body fluids and manifestations of its effects. Dr.T.V.Rao MD
Pathogens damage tissue in a variety of ways * *e.g., LPS; a polyclonal B cell activator, also see next slide Dr.T.V.Rao MD
Pattern of Antibody production. • A Lag Phase • A Log Phase raise of antibody levels, • Plateau • A phase of Decline. Dr.T.V.Rao MD
Primary and Secondary Immune Responses • A single injection of antigen helps in sensitizing or priming of immunocpompent cell producing particular antibody than in the actual elaboration of high levels of antibody. • Effective levels of antibody are usually induced by only subsequent injection of antigens. Dr.T.V.Rao MD
Booster Dose • The antibody response to an initial antigenic stimuli differs qualitatively and quantitatively from response to subsequent stimuli with the same antigen • The former primary response and later secondary response Dr.T.V.Rao MD
Primary and Secondary Response • The primary response is slow, sluggish and short lived with long lag phase and does not persist for long time • The secondary response is prompt powerful and prolonged with short or negligible lag phase and with higher level of antibodies Dr.T.V.Rao MD
Types of Antibody Response, • Initial Antigenic Stimulus (Primary Response Ig M • Response is slow and short lived, • Secondary Response Ig G • Response is Prompt ,Powerful and Prolonged Higher level of Antibodies and Lasts longer, Dr.T.V.Rao MD
How long a Antibody be active • The duration of the lag phase and persistence of the antibody dependent on the nature of the antigen • In diphtheria toxoid the lag phase in the primary response may be long as 2 -3 weeks • In pneumococcal polysaccharides antigens the antibodies are detected in few hours Dr.T.V.Rao MD
Priming and Booster doses • The first injection is known as priming dose and subsequent injection as booster dose. • With live vaccines a single dose is sufficient a single dose is sufficient as multiplication of the organisms in the body provides a continuous antigenic stimulus that acts as both the priming and booster dose Dr.T.V.Rao MD
Fate of Antigens • Depends on the physical and chemical nature of antigens, dose and route of entry • Whether induced primarily or secondarily • The antigens introduced by IV are rapidly localized in the spleen, liver, bone marrow kidney and lungs • Broken down by RES cells excreted in urine • About 70 – 80 % eliminated in one or two days Dr.T.V.Rao MD
Fate of Antigens • When antigens are introduced by subcutaneously are mainly localized in the draining lymph nodes only small amounts being found in the spleen • The pariculate antigens are removed from circulation in two phase – the first is antigens are engulfed by phagocytic cells broken down and eliminated Dr.T.V.Rao MD
Fate of Antigen • With the appearance of specific antibody the phase of immune elimination begins • The antigen and antibody complexes are rapidly phagocytized results in disappearance of antigen from circulation Dr.T.V.Rao MD
Immunoglobulin controlling genes and Generation of Diversity. • Genes control Antibody production and Diversity, • V and C regions • Kappa light chain / Lambda light chain • Rearrangements produce enormous diversity variety of Immunoglobulin • Combinations produce random selections. Dr.T.V.Rao MD
Immunoglobulin Switching. • Ig M specific for Antigen is produced. • Switch to others Ig G - Ig A -Ig E But retain the same specificity, But carry different Biological activities Dr.T.V.Rao MD
Relation of Dose and Nature of Antigen to Antibody production. • Single Dose Sensitizing. • Subsequent Dose More effective. • Non Living Vaccines multiple doses. • Living Vaccines one Dose is productive. • Fate of Antigen I V eliminate faster, in 2-3 days, in spleen. SC Lymph nodes Little in spleen Engulfed by Phagocytes Broken Down and eliminated. Dr.T.V.Rao MD
Fate of Antigen in the Host • Ag+Ab from complexes and Phagocytes will engulf and Disappear -- Immune Elimination. Immune Complexes can cause damage. Proteins eliminated in 1-2 weeks, Polysaccharides months to years. Pneumococcal polysaccharides up to 20 years. Dr.T.V.Rao MD
Production of Antibodies. • Immune Responses to Antigen, • Antigen Presenting Cells APC Macrophages Dendritic Cells T and B Lymphocytes, Capture by APC ( Proteins RBC ) T Cell take active part. T Cell Independent - Polysaccharides. Dr.T.V.Rao MD
Production of Antibodies needs help and coordination with other structures • CD4 Helper cells MHC II • CD8 Cytotoxic cells MHC • TH cells require two signals IL1 • Next produce IL2 Produce cytokines IL4 IL5 IL6 B cells stimulated Produce antibody producing plasma cells produced Dr.T.V.Rao MD
Factors Influencing Antibody production Dr.T.V.Rao MD
Factors Influencing Antibody Production • Under genetic control, • May be responder or Non responder.- defines the capacity of the individual to respond or not respond • Ir (Immune response genes) control this property. • Age The embryos is immunologic ally immature During the embryonic life the developing lymphoid cells come into contact with all the tissue antigens of the body released by cellular breakdown – lead to elimination of self antigens Dr.T.V.Rao MD
Immunity in Neonates Early mechanisms of self tolerance. -> 3-6 months Maternal antibodies, Ig G 5-7 years Ig A 10-15 years B cell responses to most proteins and other T cells dependent develop early. The responses to Polysaccharide and other T cell independent antigens develop later. Dr.T.V.Rao MD
Humoral Immunityin vivo uses • Immunoglobulin IgA can stop colonization of mucosal surface. • It interferes with the attachment molecular adhesions present on the bacterial surface. • Bacterial exotoxins are inhibited – as the antibodies can prevent interaction of enzymes with substrate. Dr.T.V.Rao MD
Humoral immunityin vivo uses • Antibodies can kill bacteria. • Antibodies can affect the specific transport systems and deprive the energy needs of the bacteria. • Affect the motility • Reduces the invasion • Antibodies can cause agglutination • Stimulate the phagocytosis, and complement activity. Dr.T.V.Rao MD
Other Factors influencing the Antibody production • Nutrition Malnutrition Humoral reduced, CMI reduced Route of administration Large particles – increased. Application to skin CMI Deltoid more effective Dr.T.V.Rao MD
Other factors, • Size and Dose has relation • Massive Dose paralysis. • Anamnestic reaction • Administration of Multiple antigens Triple antigen, Freund’s Adjuvant. Increases with Tubercle Bacilli Dr.T.V.Rao MD
Uses of Administration of Antibodies • Passive administration of Antibodies eg Hyper immune globulins, Sensitization issues in Rh negative mothers. The effect occurs due to feedback mechanism The antibody may also combine with antigen and prevent its availability for the immunocompetent cells. Rh –ve mother + Rh+ ve fetus Administration of Anti-Rh globulin immediately following delivery Dr.T.V.Rao MD
Administration of Immunoglobulin's • IV administration has immunomodulation effect • Administered in Thrombocytopenia's, and autoimmune hemolytic anemia. Dr.T.V.Rao MD
Adjuvants • Defined as substance that enhances the immunogenicity of an antigen. • Eg Aluminum hydroxide or phosphate • Freund’s incomplete adjuvant – Incorporation of protein antigen in water phase of water in oil emulsion, it causes delay of release of antigen from the site of injection and prolong the antigenic stimulus. • Freund’s complete adjuvant – contains also the suspension of killed tubercle bacilli. • The effect is due to MDP ( muramyl dipeptide ) Dr.T.V.Rao MD